wcDNA vs. cfDNA mNGS: A Comprehensive Comparison for Pathogen Identification in Clinical and Research Applications
Metagenomic Next-Generation Sequencing (mNGS) has revolutionized pathogen detection, yet the optimal choice of genetic material—whole-cell DNA (wcDNA) or cell-free DNA (cfDNA)—remains a critical methodological question.
wcDNA vs. cfDNA mNGS: A Comprehensive Comparison for Pathogen Identification in Clinical and Research Applications
Abstract
Metagenomic Next-Generation Sequencing (mNGS) has revolutionized pathogen detection, yet the optimal choice of genetic material—whole-cell DNA (wcDNA) or cell-free DNA (cfDNA)—remains a critical methodological question. This article provides a definitive comparison for researchers and drug development professionals, synthesizing the latest evidence from 2025 and 2024. We explore the foundational principles of both approaches, detail their specific applications across diverse sample types like bronchoalveolar lavage fluid (BALF), cerebrospinal fluid (CSF), and blood, and address key troubleshooting and optimization strategies to overcome challenges like high host DNA background. Finally, we present a rigorous validation and comparative analysis, evaluating the sensitivity, specificity, and clinical performance of wcDNA and cfDNA mNGS for detecting bacteria, viruses, fungi, and intracellular pathogens, empowering informed methodological selection for diagnostic development and biomedical research.
Decoding the Core Technologies: An Introduction to wcDNA and cfDNA in mNGS
Whole-cell DNA (wcDNA) refers to the total genomic DNA extracted from intact microbial cells within a sample. Unlike microbial cell-free DNA (cfDNA), which is derived from extracellular DNA fragments, wcDNA provides a comprehensive genetic snapshot of the viable microbial community, making it a fundamental component in metagenomic studies of host-associated and environmental microbiomes [1]. The analysis of wcDNA via metagenomic next-generation sequencing (mNGS) offers researchers a powerful tool for pathogen identification, microbial ecology studies, and therapeutic development by capturing genetic material from intact microorganisms.
The distinction between wcDNA and cfDNA is particularly crucial in microbiome research and clinical diagnostics, where understanding the source and representation of genetic material can significantly impact data interpretation. wcDNA extraction involves lysing intact cells to release genomic DNA, thereby representing the living microbial population at the time of sample collection [2]. This comprehensive representation makes wcDNA especially valuable for research requiring complete microbial profiling, including studies of inflammatory bowel disease (IBD) where bacterial species such as Enterococcus faecium and Bifidobacterium spp. are enriched, and Escherichia coli with its associated antibiotic resistance genes are characteristic of Crohn's disease [3]. This guide provides a detailed comparison of wcDNA methodologies, extraction protocols, and performance characteristics relative to cfDNA alternatives for pathogen identification research.
Sourcing and Extraction of wcDNA
Whole-cell DNA can be sourced from diverse clinical and environmental samples, each presenting unique challenges and considerations for optimal DNA recovery. Common sources include:
- Bodily fluids: Bronchoalveolar lavage fluid (BALF), blood, saliva, urine, and other sterile body fluids [2] [1]. These samples typically contain inhibitors like heme or mucin that require specialized lysis approaches.
- Tissue samples: Liver, muscle, heart, brain, and other tissues often necessitate mechanical disruption through homogenization or bead beating due to their fibrous and tough nature [4].
- Stool samples: Provide access to complex gut microbial communities but require stabilization media to prevent degradation from environmental factors and bacterial growth [4] [3].
- Swab samples: Buccal or dry swabs that may contain high concentrations of bacteria and contaminants, requiring optimized drying, storage, and extraction protocols [4].
- Environmental samples: Filter membranes from water sources requiring specialized processing for long DNA fragment acquisition [5].
- Formalin-fixed paraffin-embedded (FFPE) samples: Among the most challenging sources, requiring dewaxing and deparaffinization steps before nucleic acid access [4].
The selection of appropriate sample types directly impacts wcDNA yield and quality, with each source demanding tailored extraction approaches to address specific compositional characteristics and potential inhibitors.
Extraction Methodologies and Protocols
Effective wcDNA extraction follows a fundamental sequence: cellular lysis, binding or precipitation of DNA, washing of bound DNA, and elution or resuspension in a working buffer [4]. The following section details specific protocols and methodologies optimized for wcDNA recovery.
Standardized wcDNA Extraction from Body Fluids
For body fluid samples such as BALF, a standardized protocol yields high-quality wcDNA suitable for downstream mNGS applications [2] [1]:
- Sample Preparation: Begin with direct use of BALF sample without centrifugation.
- Mechanical Lysis: Add two 3-mm nickel beads to the sample and shake at 3,000 rpm for 5 minutes to facilitate complete cell lysis.
- DNA Extraction: Use the Qiagen DNA Mini Kit according to manufacturer's protocol [2].
- Quality Assessment: Verify DNA concentration and quality using spectrophotometric methods (e.g., Nanodrop) with optimal A260/A280 ratios typically ≥1.6 [4].
This method emphasizes mechanical disruption to ensure comprehensive cell lysis, particularly important for robust bacterial cell walls in microbial samples.
Phenol-Chloroform-Isoamyl Alcohol Method for Environmental Samples
For environmental DNA samples preserved on filter membranes, an organic isolation method optimized for long fragment acquisition provides superior results [5]:
- Filter Preparation: Place ½ filter membrane in a 1.5 mL Eppendorf tube with 900 µL of Longmire buffer. For filters preserved in 96% ethanol, dry completely before transfer to Longmire buffer.
- Heat Shock Treatment: Incubate at 95°C for 10 minutes, then cool to room temperature.
- Vortexing: Mix for 5-10 seconds to ensure homogenization.
- Enzymatic Digestion: Add 9 µL of Proteinase K (20 mg/mL) for a final concentration of 0.2 mg/mL. Vortex for 30 seconds and incubate for 2 hours at 56°C.
- Organic Extraction:
- Add 800 µL of phenol-chloroform-isoamyl alcohol (25:24:1, pH 8), vortex until homogenized, and centrifuge for 5 minutes at 13,300 rpm.
- Transfer the upper aqueous phase to a new tube containing 800 µL of chloroform-isoamyl alcohol (24:1), vortex, and centrifuge again.
- DNA Precipitation: Transfer the upper phase to a new tube, add 800 µL of isopropanol and 34 µL of 5M NaCl. Mix by inversion and incubate overnight at 4°C.
- Washing and Elution: Centrifuge for 30 minutes at 13,300 rpm, pour off the supernatant, wash with 800 µL of 80% iced ethanol, and repeat centrifugation. Dry the pellet and resuspend in 50-75 µL of ultrapure water at 37°C.
This method maximizes DNA recovery from challenging environmental samples while preserving fragment length, crucial for long-read sequencing technologies.
Magnetic Silica Bead-Based Rapid Extraction
Recent advancements have led to the development of SHIFT-SP (Silica bead-based High-yield Fast Tip-based Sample Prep), a magnetic bead-based method that significantly reduces extraction time while maintaining high yield [6]:
- Binding Optimization: Use lysis binding buffer (LBB) at pH 4.1 instead of pH 8.2 to enhance DNA binding to silica beads by reducing electrostatic repulsion.
- Tip-Based Binding: Employ pipette tip-based mixing (aspirating and dispensing repeatedly) for 1-2 minutes instead of orbital shaking, increasing binding efficiency from ~47% to ~85% for 100 ng input DNA.
- Bead Volume Adjustment: Utilize 30-50 µL of magnetic silica beads for higher DNA inputs (1000 ng), achieving 92-96% binding efficiency.
- Elution Conditions: Elute bound DNA using optimized buffers at appropriate pH and temperature to maximize recovery.
- Process Completion: Entire process requires only 6-7 minutes compared to 25-40 minutes for conventional column or bead-based methods [6].
This rapid, high-yield method is particularly valuable for clinical diagnostics where turnaround time is critical, and has demonstrated effectiveness with low microbial concentrations from enriched whole blood.
wcDNA Performance Comparison with cfDNA
Methodological Comparison and Detection Efficacy
Multiple studies have directly compared the performance characteristics of wcDNA and cfDNA for mNGS-based pathogen detection, revealing significant differences in their applications and effectiveness.
Table 1: Comprehensive Comparison of wcDNA vs. cfDNA mNGS Performance
| Performance Metric | wcDNA mNGS | cfDNA mNGS | Clinical Implications |
|---|---|---|---|
| Host DNA Proportion | 84% [2] | 95% [2] | Lower host DNA in wcDNA improves microbial detection sensitivity |
| Concordance with Culture | 63.3% [2] | 46.7% [2] | wcDNA shows better alignment with gold standard methods |
| Detection Rate | 83.1% [1] | 91.5% [1] | cfDNA demonstrates superior overall detection capability |
| Fungi Detection | 19.7% exclusive detection [1] | 31.8% exclusive detection [1] | cfDNA more effective for fungal identification |
| Virus Detection | 14.3% exclusive detection [1] | 38.6% exclusive detection [1] | cfDNA superior for viral pathogen detection |
| Intracellular Microbes | 6.7% exclusive detection [1] | 26.7% exclusive detection [1] | cfDNA better for obligate intracellular pathogens |
| Bacterial Detection Consistency with Culture | 70.7% [2] | Not reported | wcDNA more reliable for bacterial pathogen detection |
| Sensitivity | 74.07% [2] | Not reported | Moderate sensitivity for pathogen detection |
| Specificity | 56.34% [2] | Not reported | Compromised specificity requires careful result interpretation |
The data reveals a fundamental divergence in application strengths: wcDNA mNGS demonstrates superior performance for bacterial detection with better concordance to culture methods, while cfDNA mNGS excels in detecting fungi, viruses, and intracellular microbes with low loads [2] [1].
Microbial Community Representation
The choice between wcDNA and cfDNA significantly influences the resulting microbial community profile and subsequent data interpretation in research settings.
Table 2: Microbial Community Representation in wcDNA vs. cfDNA
| Representation Aspect | wcDNA mNGS | cfDNA mNGS | Research Implications |
|---|---|---|---|
| Biodiversity Assessment | Represents intact cellular community | Skewed toward lysing or degrading organisms | wcDNA more accurate for viable community structure |
| Bacterial Pathogen Detection | Enhanced detection of abundant bacteria | May miss some intact bacteria | wcDNA preferable for bacterial infection studies |
| Low Load Microbe Detection | Lower sensitivity for microbes with low abundance | Higher sensitivity for fungi, viruses with low loads | Choice depends on target pathogen type |
| Antibiotic Resistance Gene Detection | Effective for associated resistance genes | May miss some intracellular resistance markers | wcDNA better for resistome analysis in bacterial pathogens |
| Functional Gene Analysis | Comprehensive genomic representation | Fragmented genetic information | wcDNA superior for functional potential assessment |
wcDNA provides a more accurate representation of the viable microbial community, as demonstrated in gut microbiome studies where wcDNA analysis revealed distinct bacteriome signatures between ulcerative colitis and Crohn's disease patients, including enriched Enterococcus faecium in both diseases and Escherichia coli characteristic of CD [3]. This representation is crucial for understanding functional potential and microbial ecology in research settings.
Research Reagent Solutions for wcDNA Studies
Successful wcDNA extraction and analysis requires carefully selected reagents and kits optimized for different sample types and research objectives.
Table 3: Essential Research Reagents for wcDNA Extraction and Analysis
| Reagent/Kit | Primary Function | Application Context | Sample Types |
|---|---|---|---|
| Qiagen DNA Mini Kit | Standardized silica-column DNA purification | Routine wcDNA extraction from various samples | Body fluids, tissues, cultures [2] |
| MagMAX DNA Multi-Sample Ultra 2.0 | Magnetic bead-based DNA purification | High-throughput automated extraction | Blood, bone marrow, saliva, tissue [4] |
| Proteinase K | Protein digestion for cell lysis | Enzymatic disruption of cellular structures | Tough samples (tissue, spores) [5] |
| Phenol-Chloroform-Isoamyl Alcohol | Organic nucleic acid separation | Maximum DNA recovery, long fragments | Environmental samples, difficult tissues [5] |
| RNase A | RNA degradation | Reduction of RNA contamination | Tissue samples with high RNA content [4] |
| Lysis Binding Buffer (pH 4.1) | Enhanced DNA binding to silica | Magnetic bead-based rapid extraction | All sample types with low input DNA [6] |
| EDTA | Demineralization and nuclease inhibition | Bone samples and nuclease-rich samples | Forensic samples, ancient DNA, bone [7] |
| PVP (Polyvinylpyrrolidone) | Polyphenol binding | Plant samples with high polyphenols | Plant tissues, soil samples [4] |
Selection of appropriate reagents depends on sample characteristics, downstream applications, and throughput requirements. For clinical diagnostics with body fluids, optimized kits like the Qiagen DNA Mini Kit provide reproducibility, while research involving challenging samples may require specialized additives like PVP for plant materials or EDTA for demineralization of tough matrices [4] [7].
Experimental Workflows and Signaling Pathways
wcDNA mNGS Experimental Workflow
The complete workflow for wcDNA-based metagenomic analysis involves multiple critical steps from sample collection to data interpretation, each requiring careful optimization to ensure representative microbial community data.
Figure 1: wcDNA mNGS Experimental Workflow. This diagram illustrates the comprehensive process from sample collection to data interpretation, highlighting key steps including mechanical lysis and quality control specific to wcDNA analysis.
Method Selection Decision Pathway
Choosing between wcDNA and cfDNA approaches requires careful consideration of research goals, sample types, and target microorganisms, as each method offers distinct advantages for specific applications.
Figure 2: Method Selection Decision Pathway. This flowchart provides a systematic approach for selecting between wcDNA and cfDNA methods based on research objectives, sample characteristics, target microbes, and resource considerations.
Whole-cell DNA extraction and analysis represents a cornerstone approach in microbial metagenomics, providing researchers with a comprehensive tool for assessing viable microbial communities. The methodological comparisons presented in this guide demonstrate that wcDNA mNGS offers distinct advantages for bacterial detection and community structure analysis, while cfDNA excels in identifying intracellular pathogens, fungi, and viruses with low microbial loads.
The choice between wcDNA and cfDNA methodologies should be guided by specific research objectives, sample types, and target microorganisms. For drug development professionals and clinical researchers, understanding these distinctions is crucial for appropriate experimental design and accurate data interpretation. As metagenomic technologies continue to evolve, the strategic application of wcDNA analysis will remain essential for advancing our understanding of microbiome dynamics in human health, disease pathogenesis, and therapeutic development.
Future methodological developments will likely focus on reducing host DNA contamination in wcDNA extracts, enhancing sensitivity for low-abundance taxa, and streamlining automated workflows for high-throughput applications. By leveraging the appropriate extraction methodologies and analytical frameworks outlined in this guide, researchers can maximize the research value of wcDNA in diverse microbiological studies.
Cell-free DNA (cfDNA) refers to short fragments of extracellular nucleic acids circulating in bodily fluids such as blood plasma, cerebrospinal fluid, and bronchoalveolar lavage fluid. Since its initial discovery in human blood by Mandel and Metais in 1948 [8] [9], cfDNA analysis has evolved into a powerful clinical tool across medical specialties. In infectious disease diagnostics, the application of metagenomic next-generation sequencing (mNGS) to cfDNA has emerged as a particularly promising approach for pathogen identification, offering a non-invasive method to detect microbial sequences without the need for invasive tissue biopsies [9].
The fundamental distinction in mNGS testing approaches lies between microbial cell-free DNA (mcfDNA) sequencing and whole-cell DNA (wcDNA) sequencing. The wcDNA approach extracts genetic material from intact microorganisms and human cells in a sample, while cfDNA protocols specifically target extracellular DNA released into bodily fluids through various biological processes [2] [1]. Understanding the biological origins and characteristics of cfDNA is essential for optimizing its diagnostic application and interpreting results accurately within the context of pathogen detection.
Biological Origins of Cell-Free DNA
Primary Mechanisms of cfDNA Release
The pool of cfDNA in circulation originates through several distinct biological processes, with apoptosis and necrosis representing the most significant pathways.
Apoptosis
Apoptosis, or programmed cell death, is considered the primary source of circulating cfDNA in both healthy individuals and those with disease [8] [10]. This highly regulated process occurs continuously in the human body, with an estimated 50 to 70 billion cells undergoing apoptosis daily [8]. During apoptosis, caspase-activated DNase (CAD) and DNaseI L-3 enzymatically cleave nuclear DNA at internucleosomal linker regions, producing characteristic DNA fragments of approximately 167 base pairs in length—the size classically associated with mononucleosomes [8]. Recent genetic evidence from CRISPR screening studies has definitively confirmed apoptosis as a major mediator of cfDNA release, identifying genes involved in apoptotic processes as primary effectors [10].
Necrosis
In contrast to the controlled process of apoptosis, necrosis represents accidental cell death resulting from pathological insults such as ischemia, trauma, or toxicity. This unregulated process leads to cellular swelling and membrane rupture, releasing larger, more variable DNA fragments that often exceed 1000 base pairs in length [8] [10]. While these larger fragments are susceptible to rapid degradation by plasma nucleases, they nevertheless contribute to the circulating cfDNA pool, particularly in conditions involving significant tissue damage [8].
Other Contributing Mechanisms
Additional processes contribute to cfDNA populations, though to a lesser extent. Active secretion of DNA through extracellular vesicles represents a potential mechanism, though the exact significance remains debated [10]. Erythroblast enucleation during red blood cell maturation has also been hypothesized as a cfDNA source, though experimental evidence remains limited [8].
cfDNA Fragment Characteristics and Clearance
Regardless of origin, cfDNA fragments typically exist as double-stranded molecules ranging between 100-200 base pairs, though larger fragments have been reported [8]. Following release into circulation, cfDNA exhibits a remarkably short half-life, estimated between 16 minutes to 2.5 hours [11]. Clearance occurs primarily through degradation by plasma nucleases, with the liver, spleen, and kidneys also contributing to elimination [8]. This rapid turnover makes cfDNA an excellent dynamic biomarker for monitoring disease progression or treatment response.
Figure 1: Biological Origins and Clearance Pathways of Cell-Free DNA. This diagram illustrates the primary cellular sources of cfDNA, including apoptosis and necrosis, the characteristic fragment sizes produced by each mechanism, and the major clearance pathways that determine cfDNA half-life in circulation.
Comparative Analysis: wcDNA mNGS vs. cfDNA mNGS for Pathogen Detection
Technical Workflows and Methodological Considerations
The fundamental distinction between wcDNA and cfDNA mNGS approaches lies in sample processing and DNA extraction procedures.
wcDNA mNGS Protocol: This approach processes the entire clinical sample, typically employing mechanical (e.g., bead-beating) or enzymatic lysis to liberate genomic DNA from both host cells and intact microorganisms [2] [1]. The resulting DNA represents the complete genetic material present in the sample, including high molecular weight genomic DNA from viable organisms.
cfDNA mNGS Protocol: This method begins with centrifugation to generate a low-cellularity supernatant, followed by extraction of extracellular DNA from this supernatant using specialized kits designed to capture short nucleic acid fragments [2] [1]. This process selectively enriches for DNA released into bodily fluids through cell death or active secretion while depleting intact cellular material.
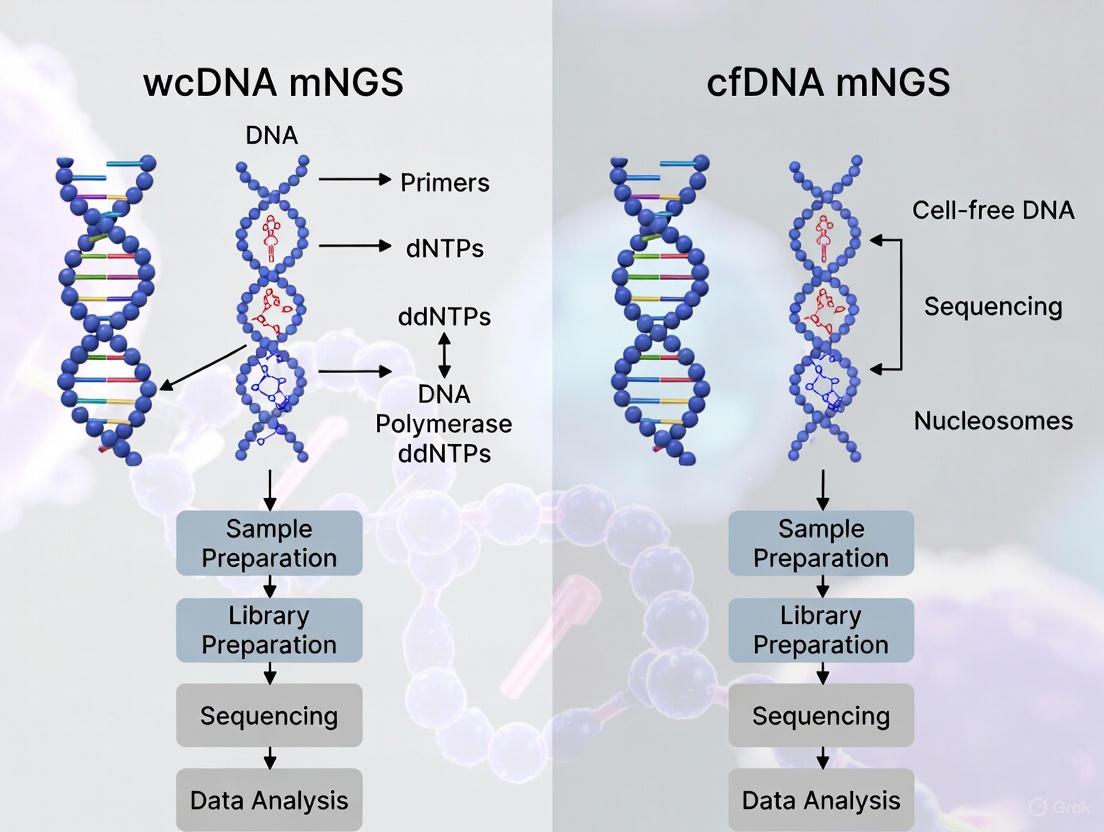
Figure 2: Comparative Workflows for wcDNA and cfDNA mNGS Testing. This diagram illustrates the distinct sample processing pathways for whole-cell DNA versus cell-free DNA metagenomic next-generation sequencing, highlighting key methodological differences from sample collection through library preparation.
Performance Comparison in Clinical Studies
Recent head-to-head comparisons have revealed significant differences in the diagnostic performance of wcDNA versus cfDNA mNGS approaches across various clinical scenarios and sample types.
Table 1: Comparative Performance of wcDNA mNGS vs. cfDNA mNGS in Body Fluid Samples
| Performance Metric | wcDNA mNGS | cfDNA mNGS | Study Details |
|---|---|---|---|
| Sensitivity | 74.07% | Not reported | Compared to culture in body fluid samples (n=125) [2] |
| Specificity | 56.34% | Not reported | Compared to culture in body fluid samples (n=125) [2] |
| Concordance with Culture | 63.33% (19/30) | 46.67% (14/30) | Direct comparison in 30 body fluid samples [2] |
| Host DNA Proportion | Mean 84% | Mean 95% (p<0.05) | Significantly lower host DNA in wcDNA [2] |
| Detection Rate in BALF | 83.1% | 91.5% | Pulmonary infections (n=130) [1] |
| Total Coincidence Rate in BALF | 63.9% | 73.8% | Compared to composite clinical diagnosis [1] |
Table 2: Pathogen-Type Detection Capabilities of wcDNA vs. cfDNA mNGS
| Pathogen Category | Exclusively Detected by wcDNA mNGS | Exclusively Detected by cfDNA mNGS | Clinical Implications |
|---|---|---|---|
| Fungi | 19.7% (13/66) | 31.8% (21/66) | cfDNA superior for fungal detection [1] |
| Viruses | 14.3% (10/70) | 38.6% (27/70) | cfDNA superior for viral detection [1] |
| Intracellular Microbes | 6.7% (2/30) | 26.7% (8/30) | cfDNA better for obligate intracellular pathogens [1] |
| Consistency with 16S rRNA NGS | 70.7% (29/41) | Not reported | wcDNA shows better concordance with 16S method [2] |
The differential performance between these approaches reflects their fundamental biological distinctions. The wcDNA mNGS demonstrates strength in detecting a broad spectrum of pathogens, particularly extracellular bacteria, with higher concordance to traditional culture methods [2]. In contrast, cfDNA mNGS excels in identifying intracellular pathogens, fungi, and viruses, likely because these microorganisms release their nucleic acids into host circulation during infection or through host cell lysis [1].
Advantages and Limitations in Clinical Practice
Each approach presents a distinct profile of strengths and limitations that must be considered in diagnostic applications.
wcDNA mNGS Advantages: This method provides more comprehensive genomic information, potentially enabling strain-level characterization and detection of antimicrobial resistance genes due to the presence of intact microbial genomes [9]. It typically generates higher microbial reads per million (RPM), with one study reporting an average of 2,359 RPM for wcDNA versus 95 RPM for cfDNA [9]. The approach also demonstrates higher sensitivity for certain bacterial pathogens and better correlation with culture results for common microorganisms [2].
wcDNA mNGS Limitations: The presence of high levels of background host DNA (approximately 84% of total sequences) can reduce sensitivity for low-abundance pathogens unless host depletion strategies are employed [2] [9]. The extraction process may be harsher, potentially leading to DNA fragmentation, and the approach may be less effective for detecting pathogens that are primarily intracellular or that release their DNA into circulation [1].
cfDNA mNGS Advantages: This method excels for detecting intracellular pathogens, fungi, and viruses, with significantly higher exclusive detection rates for these categories of microorganisms [1]. The minimal invasiveness of blood-based testing enables serial monitoring of infection dynamics and treatment response. The approach also demonstrates higher overall detection rates in respiratory infections (91.5% vs. 83.1% for wcDNA) [1].
cfDNA mNGS Limitations: Microbial cfDNA typically represents an extremely small fraction of total cfDNA, creating challenges for detection and increasing vulnerability to contamination [9]. The fragmented nature of cfDNA limits opportunities for strain-level characterization or comprehensive resistance profiling. The approach shows lower concordance with culture results (46.67% vs. 63.33% for wcDNA) and may miss extracellular pathogens that do not release significant DNA into circulation [2].
Essential Research Reagents and Methodologies
Table 3: Essential Research Reagents for wcDNA and cfDNA mNGS Workflows
| Reagent/Category | Specific Examples | Function in Workflow | Application |
|---|---|---|---|
| DNA Extraction Kits | QIAamp DNA Micro Kit [2] | Extraction of high-quality DNA from clinical samples | Both wcDNA & cfDNA |
| cfDNA Specialized Kits | VAHTS Free-Circulating DNA Maxi Kit [2] | Optimized extraction of short cfDNA fragments | cfDNA mNGS |
| Library Preparation | QIAseq Ultralow Input Library Kit [1] | Library construction from low-input DNA | Both wcDNA & cfDNA |
| Host Depletion | Devin Microbial DNA Enrichment Kit [9] | Selective removal of human DNA to enhance microbial signal | Primarily wcDNA |
| Sequencing | Illumina NovaSeq platform [2] | High-throughput sequencing | Both wcDNA & cfDNA |
| Bioinformatics | Pavian, Bowtie2, Custom pipelines [2] [1] | Taxonomic classification, host sequence removal | Both wcDNA & cfDNA |
Clinical Applications and Future Directions
The complementary strengths of wcDNA and cfDNA mNGS suggest context-specific applications in clinical practice. The wcDNA mNGS may be preferred for samples from sterile sites where comprehensive pathogen characterization is required, or when antimicrobial resistance profiling is clinically essential [9]. Conversely, cfDNA mNGS shows particular promise for blood-based testing in febrile immunocompromised patients, suspected deep-seated infections, and cases where intracellular pathogens are considered likely [1] [9].
In oncology, cfDNA analysis has established utility for non-invasive tumor profiling and monitoring, with applications now extending to infectious disease diagnostics [11] [12]. The high concordance between tumor mutations detected in tissue biopsies and plasma cfDNA (median 88% for oncogenic mutations) demonstrates the reliability of cfDNA-based approaches [12].
Future methodological developments will likely focus on hybrid approaches that leverage the strengths of both techniques. Potential innovations include parallel sequencing of both fractions, optimized host-depletion strategies for wcDNA protocols, and targeted enrichment methods to enhance sensitivity for low-abundance pathogens in cfDNA assays. As our understanding of cfDNA biology deepens and sequencing technologies evolve, mNGS-based pathogen detection promises to play an increasingly central role in clinical microbiology and infectious disease diagnostics.
The comparative analysis of wcDNA and cfDNA mNGS approaches reveals a complex landscape where each method offers distinct advantages depending on clinical context, suspected pathogen spectrum, and sample type. The wcDNA mNGS demonstrates higher sensitivity for bacterial detection and better concordance with conventional culture methods, while cfDNA mNGS excels in detecting intracellular pathogens, fungi, and viruses. Understanding the biological origins of cfDNA in apoptosis and necrosis provides crucial context for interpreting diagnostic results and optimizing test selection. As methodological refinements continue to enhance performance characteristics, both approaches will undoubtedly play increasingly important roles in the rapid, precise diagnosis of infectious diseases, ultimately supporting improved patient outcomes through targeted therapeutic interventions.
Metagenomic Next-Generation Sequencing (mNGS) has revolutionized pathogen detection by providing a hypothesis-free approach to infectious disease diagnosis. This technology enables the simultaneous identification of bacteria, viruses, fungi, and parasites directly from clinical samples without prior knowledge of the causative agent [13] [14]. The workflow encompasses a series of complex steps from sample collection to bioinformatic analysis, each critical for achieving accurate diagnostic results. Within this domain, a key methodological distinction exists between whole-cell DNA (wcDNA) mNGS, which sequences DNA from intact microbial cells, and cell-free DNA (cfDNA) mNGS, which targets freely circulating microbial nucleic acids often from plasma [14]. This guide objectively compares these approaches, detailing their workflows, performance characteristics, and applications in pathogen identification research.
Wet Lab Workflow: From Sample to Sequence
Sample Collection and Processing
The initial phase of the mNGS workflow focuses on obtaining quality specimens while minimizing exogenous contamination. Appropriate sample collection varies significantly between wcDNA and cfDNA approaches.
Sample Types: Common specimens for wcDNA mNGS include bronchoalveolar lavage fluid (BALF), sputum, tissue biopsies, and cerebrospinal fluid (CSF) [15] [16]. These samples contain intact microorganisms. For cfDNA mNGS, blood collected in specialized cell-free DNA blood collection tubes is the primary source, enabling detection of pathogen nucleic acids released into the bloodstream [14].
Nucleic Acid Extraction: Extraction methods must be optimized for different sample matrices. The wcDNA protocol typically involves mechanical or enzymatic lysis of microbial cells followed by nucleic acid purification using commercial kits [15] [17]. The cfDNA approach requires specialized extraction to isolate short, fragmented nucleic acids from plasma while excluding longer genomic DNA [14].
Host Depletion and Library Preparation
Reducing host nucleic acid background is particularly crucial for wcDNA mNGS of low-biomass infections where microbial reads may be overwhelmed by host DNA.
Host Depletion Methods: Techniques include saponin lysis of host cells, differential centrifugation, filtration, and nuclease treatment [17] [18]. For example, one respiratory sample protocol uses 0.2% saponin treatment followed by filtration through 0.22 µm filters to remove host cells and debris [18].
Library Preparation: This process converts extracted nucleic acids into sequencing-ready libraries. Methods vary by platform:
Table 1: Key Research Reagent Solutions for mNGS Workflows
| Reagent/Kit | Application | Function | Example Product |
|---|---|---|---|
| Nucleic Acid Extraction Kit | Nucleic acid purification | Isolates DNA/RNA from samples | MatriDx MD013 [15] |
| MagMAX Viral/Pathogen Kit | Nucleic acid isolation | Concentrates pathogen nucleic acids | MagMAX Viral/Pathogen Nucleic Acid Isolation Kit [17] |
| Rapid PCR Barcoding Kit | Library preparation | Tags DNA with barcodes for multiplexing | SQK-RPB114.24 [17] |
| TURBO DNase | Host depletion | Degrades residual host DNA | TURBO DNase [18] |
| Agencourt AMPure XP beads | Library clean-up | Purifies and size-selects DNA fragments | Beckman Coulter AMPure XP [17] |
Sequencing Platforms
The choice between short-read and long-read technologies significantly impacts mNGS capabilities:
Illumina (Short-Read): Provides high accuracy (Q30 >85%) but shorter read lengths (2×150 bp to 2×300 bp) [19] [13]. Ideal for high-sensitivity pathogen detection and abundance quantification.
Oxford Nanopore (Long-Read): Generates longer reads (thousands of bases) with real-time sequencing capability, enabling rapid pathogen identification [13] [18]. The portable MinION device facilitates field deployment [14].
Bioinformatic Analysis Pipeline
The computational analysis of mNGS data transforms raw sequencing reads into actionable pathogen identification through a multi-step process [19] [20].
Quality Control and Preprocessing
Initial processing ensures data integrity and removes low-quality sequences:
Quality Assessment: Tools like FastQC visualize read quality distributions, while MultiQC aggregates metrics across multiple samples [19]. Minimum thresholds typically require ≥85% of bases with Phred scores ≥30 (Q30) [19].
Adapter Trimming: Trimmomatic or KneadData remove adapter sequences and trim low-quality bases [19].
Host Sequence Removal: Alignment to host reference genomes (e.g., GRCh38) using Bowtie2, BWA, or Kraken2 eliminates residual host reads, significantly improving microbial detection sensitivity [19].
Taxonomic Classification and Functional Analysis
The core identification process involves comparing non-host reads to microbial databases:
Alignment-Based Methods: Kraken2 uses k-mer hashing for rapid taxonomic classification, while Bowtie2 provides precise alignment to reference genomes [19] [16].
Marker-Based Approaches: MetaPhlAn 4 leverages clade-specific marker genes for species-level precision [19].
Assembly-Based Methods: For novel pathogen discovery, de novo assembly with MEGAHIT or metaSPAdes reconstructs contigs and metagenome-assembled genomes (MAGs) without reference databases [19] [20].
Functional Annotation: Tools like Prokka predict open reading frames, while specialized databases (* CAZy, *MEROPS, AMRFinderPlus) identify carbohydrate-active enzymes, proteases, and antimicrobial resistance genes [19].
Table 2: Performance Comparison of mNGS Platforms and Methods
| Parameter | wcDNA mNGS (BALF/Tissue) | cfDNA mNGS (Plasma) | Conventional Methods |
|---|---|---|---|
| Sensitivity | 56.5% for pulmonary infections [16] | 63% for CNS infections [14] | 39.1% for culture [16] |
| Turnaround Time | 24-72 hours [13] | 24-72 hours [14] | 3-5 days (culture) [13] |
| Pathogen Spectrum | Comprehensive (bacteria, viruses, fungi, parasites) [15] [16] | Primarily bloodborne pathogens [14] | Target-specific |
| Host DNA Interference | High (requires depletion) [14] | Low (naturally enriched) [14] | Not applicable |
| Ability to Detect Co-infections | Excellent (7% additional cases) [18] | Moderate | Limited |
Experimental Protocols for Method Comparison
wcDNA mNGS Protocol for Respiratory Samples
This protocol is adapted from clinical studies of pulmonary cryptococcosis and lower respiratory tract infections [15] [16]:
Sample Collection: Collect ≥5 mL BALF in sterile containers and transport on dry ice within 2 hours.
DNA Extraction: Use automated systems (e.g., MatriDx MAR002) with commercial kits (e.g., MatriDx MD013) following manufacturer protocols.
Library Preparation: Fragment DNA to 200-500 bp, ligate platform-specific adapters, and amplify with barcoded primers.
Sequencing: Load libraries onto Illumina (NextSeq500) or Nanopore (MinION) platforms to generate 10-20 million reads per sample.
Quality Control: Include negative (sterile water) and positive controls with spike-in molecules to monitor contamination and sensitivity.
cfDNA mNGS Protocol for Blood Samples
This protocol is adapted from liquid biopsy approaches for pathogen detection [14]:
Plasma Separation: Centrifuge blood collection tubes at 1600×g for 10 minutes within 2 hours of collection.
cfDNA Extraction: Use specialized cell-free DNA extraction kits to isolate short-fragment DNA from 1-5 mL plasma.
Library Construction: Employ unique molecular identifiers to distinguish true microbial signals from background noise.
Sequencing: Sequence to higher depth (20-30 million reads) to compensate for lower pathogen DNA concentration.
Bioinformatic Filtering: Apply stringent thresholds to distinguish circulating microbial DNA from contamination.
Performance Comparison and Applications
Diagnostic Performance Metrics
Clinical validation studies demonstrate the complementary strengths of wcDNA and cfDNA mNGS approaches:
Sensitivity and Specificity: wcDNA mNGS shows superior sensitivity (56.5%) for localized respiratory infections compared to conventional methods (39.1%) [16]. cfDNA mNGS achieves 63% diagnostic yield in central nervous system infections where conventional methods fall below 30% [14].
Turnaround Time: mNGS significantly reduces time to results (1.00 day vs. 4.50 days for culture) and accelerates clinical decision-making (3.50 days vs. 9.00 days from admission) [15].
Co-infection Detection: mNGS identifies polymicrobial infections in 7% of cases missed by routine tests, including influenza C virus and Sapporovirus [18].
Unique Applications
wcDNA mNGS Applications:
cfDNA mNGS Applications:
- Disseminated and bloodstream infections
- Culture-negative sepsis
- Infections in critically ill patients
- Monitoring treatment response [14]
The mNGS workflow represents a paradigm shift in pathogen identification, offering unprecedented capabilities for comprehensive microbial detection. The choice between wcDNA and cfDNA approaches depends on clinical context, with wcDNA excelling in localized infections and cfDNA providing value for systemic illnesses. As sequencing technologies advance and bioinformatic tools become more sophisticated, mNGS is poised to become an integral component of precision infectious disease management, particularly for complex diagnostic challenges. Future developments in standardization, reimbursement models, and point-of-care applications will determine the broader implementation of these powerful diagnostic tools across diverse healthcare settings.
Comparative Advantages and Inherent Limitations of Each DNA Source
The choice between whole-cell DNA (wcDNA) and cell-free DNA (cfDNA) as the optimal input for metagenomic next-generation sequencing (mNGS) in pathogen identification is a pivotal decision that significantly impacts diagnostic outcomes. Current research reveals that this choice is highly context-dependent, with each source demonstrating distinct advantages and limitations influenced by sample type, target pathogens, and laboratory workflow. wcDNA mNGS generally offers higher sensitivity for common bacterial pathogens in sterile body fluids. In contrast, cfDNA mNGS shows superior performance for detecting intracellular microbes, fungi, and viruses, particularly from samples like bronchoalveolar lavage fluid (BALF). This guide provides a detailed, evidence-based comparison of these two methods to inform researcher selection for specific diagnostic scenarios.
Performance Data at a Glance
The following tables summarize key comparative findings from recent clinical studies across various sample types.
Table 1: Overall Diagnostic Performance Across Sample Types
| Sample Type | Metric | wcDNA mNGS | cfDNA mNGS | Reference Standard | Citation |
|---|---|---|---|---|---|
| Clinical Body Fluids (n=125) | Sensitivity | 74.07% | - | Culture | [2] |
| Specificity | 56.34% | - | Culture | [2] | |
| Concordance with Culture | 63.33% (19/30) | 46.67% (14/30) | Culture | [2] | |
| Pulmonary Infections (BALF, n=130) | Detection Rate | 83.1% | 91.5% | Conventional Methods + Clinical Diagnosis | [1] |
| Total Coincidence Rate | 63.9% | 73.8% | Conventional Methods + Clinical Diagnosis | [1] | |
| Non-Neutropenic Pulmonary Aspergillosis (BALF) | Clinical Value (AUC) | - | Superior to wcDNA | Conventional Microbiological Tests | [21] |
Table 2: Pathogen-Type Detection Capabilities
| Pathogen Type | Detection Capability | Key Findings | Sample Type | Citation |
|---|---|---|---|---|
| Fungi, Viruses, Intracellular Microbes | Higher with cfDNA mNGS | 31.8% of fungi, 38.6% of viruses, 26.7% of intracellular microbes detected only by cfDNA mNGS. | BALF | [1] |
| Gram-positive Bacteria | Variable; can be lower with cfDNA mNGS | In preservation fluids, mNGS (cfDNA-based) detected only 22.2% (2/9) of culture-positive Gram-positive bacteria. | Organ Preservation Fluids | [22] [23] |
| Atypical Pathogens | Effectively detected by mNGS | Mycobacterium, Clostridium tetanus, and parasites detected solely via mNGS. | Organ Preservation & Drainage Fluids | [22] [23] |
Experimental Protocols and Workflows
Understanding the methodological differences is crucial for interpreting performance data and selecting the appropriate protocol.
Core Protocol for wcDNA and cfDNA Extraction from Body Fluids
A seminal study comparing both methods on the same 125 clinical body fluid samples (pleural, pancreatic, drainage, ascites, and CSF) detailed the following protocol [2]:
- Sample Processing: A 30-minute centrifugation at 20,000 × g separates the cellular pellet from the cell-free supernatant.
- wcDNA Extraction:
- The retained precipitate is subjected to mechanical lysis (e.g., bead beating).
- DNA is then extracted from the lysed pellet using a commercial kit (e.g., Qiagen DNA Mini Kit).
- cfDNA Extraction:
- Cell-free DNA is extracted from the supernatant (e.g., 400 μL) using a specialized circulating DNA kit (e.g., VAHTS Free-Circulating DNA Maxi Kit).
- This typically involves proteinase K digestion, binding to magnetic beads, washes, and elution.
Workflow Comparison
The diagram below illustrates the key procedural differences between the wcDNA and cfDNA mNGS pathways.
Advanced Workflow: Integrated Host Depletion for wcDNA
A significant limitation of wcDNA mNGS is high background host DNA. A 2025 study evaluated a novel Zwitterionic Interface Ultra-Self-assemble Coating (ZISC)-based filtration device for host depletion prior to DNA extraction [24].
Protocol Enhancement [24]:
- Host Cell Depletion: Whole blood is passed through the ZISC filter, achieving >99% white blood cell removal while allowing unimpeded passage of bacteria and viruses.
- Microbial Enrichment: The filtered sample is centrifuged to obtain a microbial cell pellet.
- DNA Extraction and Sequencing: DNA is extracted from this enriched pellet for subsequent library preparation and sequencing.
Key Finding: This gDNA-based workflow with pre-extraction host depletion detected all expected pathogens in 100% (8/8) of clinical sepsis samples, with a tenfold increase in microbial read counts compared to unfiltered gDNA-based mNGS, and outperformed cfDNA-based mNGS in consistency [24].
The Scientist's Toolkit: Essential Research Reagents
Table 3: Key Reagents and Kits for mNGS Workflows
| Product Name | Function in Workflow | Application Note |
|---|---|---|
| Qiagen DNA Mini Kit | Extraction of high-quality genomic DNA from cellular pellets. | Standard for wcDNA extraction from various sample types [2]. |
| VAHTS Free-Circulating DNA Maxi Kit | Optimized extraction of short-fragment, low-concentration cfDNA from supernatant/plasma. | Critical for obtaining usable cfDNA templates [2]. |
| QIAseq Ultralow Input Library Prep Kit | Library construction from minimal DNA input, preserving complexity. | Suitable for both wcDNA and cfDNA libraries where input is limiting [1] [21]. |
| ZISC-Based Filtration Device (e.g., Devin) | Pre-extraction physical depletion of host white blood cells from whole blood. | Dramatically improves signal-to-noise ratio in gDNA-based mNGS for sepsis [24]. |
| QIAamp DNA Microbiome Kit | Post-extraction enzymatic depletion of host DNA via differential lysis. | An alternative method for host depletion in complex samples [24]. |
The evidence clearly indicates that neither wcDNA nor cfDNA mNGS is universally superior. The optimal choice is a strategic decision based on the clinical or research question, target pathogen, and sample matrix.
- Choose wcDNA mNGS when investigating sterile body fluid infections (e.g., abdominal), especially when targeting common bacteria, and when the workflow can be coupled with effective host depletion methods to maximize sensitivity [2] [24].
- Choose cfDNA mNGS when dealing with pulmonary infections, particularly when fungi, viruses, or intracellular pathogens (like Mycobacterium tuberculosis) are suspected, or when the pathogen load in the sample is expected to be low [1] [25] [21].
For the most critical and challenging cases, a dual approach utilizing both DNA sources may provide the most comprehensive diagnostic picture, leveraging the unique strengths of each method to overcome their respective limitations. The ongoing development of host depletion techniques continues to shift the performance landscape, making wcDNA an increasingly powerful option for blood-based diagnostics.
The Impact of Host DNA Background on Sequencing Efficiency and Diagnostic Yield
Metagenomic next-generation sequencing (mNGS) has emerged as a powerful, hypothesis-free tool for pathogen detection in clinical infectious diseases. However, its effectiveness is significantly challenged by the presence of host DNA, which can constitute up to 95-99% of the total DNA in clinical samples [2] [26]. This high host DNA background consumes valuable sequencing throughput and reduces the microbial reads available for analysis, ultimately compromising diagnostic sensitivity. Two primary approaches have been developed to address this challenge: whole-cell DNA (wcDNA) mNGS, which sequences all DNA in a sample, and cell-free DNA (cfDNA) mNGS, which specifically targets freely circulating microbial DNA fragments. This review comprehensively compares these approaches, examining their performance characteristics across different sample types and clinical scenarios to guide researchers and clinicians in test selection and optimization.
Core Concepts: wcDNA versus cfDNA mNGS
Whole-cell DNA (wcDNA) mNGS involves extracting and sequencing the complete genomic content from a clinical sample, including both intact microbial cells and human host cells. This method captures intracellular and cell-associated pathogens but also co-extracts substantial host genomic DNA, which can dominate sequencing libraries [2] [26]. Specialized host depletion strategies, such as filtration or differential lysis, can be applied to wcDNA samples to enrich microbial content before sequencing [27] [9].
Cell-free DNA (cfDNA) mNGS targets short fragments of DNA (typically <300 bp) circulating in biofluids like plasma or supernatant from centrifuged samples. These fragments are released through processes such as apoptosis, necrosis, or pathogen lysis [9]. This approach inherently avoids the high host DNA background associated with intact cells but faces different challenges related to low absolute quantities of microbial cfDNA (mcfDNA) in samples [9] [28].
Table 1: Fundamental Characteristics of wcDNA and cfDNA mNGS Approaches
| Characteristic | wcDNA mNGS | cfDNA mNGS |
|---|---|---|
| Source Material | Precipitate/cell pellet after centrifugation | Supernatant/plasma after centrifugation |
| DNA Targets | Intact microbial genomes, host genomic DNA | Microbial and host DNA fragments |
| Typical Host DNA Percentage | ~84% in body fluids [2] | Can exceed 95% [2] |
| Key Advantage | Captures intracellular pathogens; amenable to host depletion | Minimizes interference from human cells; reflects active infection |
| Primary Challenge | High host DNA background requiring depletion methods | Very low concentration of microbial targets |
The following workflow diagram illustrates the fundamental procedural differences between these two approaches:
Comparative Performance Analysis
Diagnostic Performance Across Sample Types
Multiple clinical studies have directly compared the diagnostic performance of wcDNA and cfDNA mNGS across various sample matrices, with results demonstrating significant context-dependent performance.
Table 2: Comparative Diagnostic Performance of wcDNA vs. cfDNA mNGS
| Sample Type | Performance Metric | wcDNA mNGS | cfDNA mNGS | Study |
|---|---|---|---|---|
| Body Fluids (n=125) | Concordance with culture | 63.33% (19/30) | 46.67% (14/30) | [2] |
| Sensitivity | 74.07% | Not reported | [2] | |
| Specificity | 56.34% | Not reported | [2] | |
| BALF (n=130) | Detection rate | 83.1% | 91.5% | [1] [29] |
| Total coincidence rate | 63.9% | 73.8% | [1] [29] | |
| Blood (culture-positive sepsis, n=8) | Pathogen detection rate | 100% (8/8) | Inconsistent sensitivity | [27] |
| Average microbial RPM | 9,351 (with filtration) | 95-1,488 | [27] [9] |
In body fluids, wcDNA mNGS demonstrated superior concordance with culture results (63.33% vs. 46.67%) and a sensitivity of 74.07%, though with compromised specificity (56.34%) [2]. Conversely, in bronchoalveolar lavage fluid (BALF) from patients with pulmonary infections, cfDNA mNGS showed significantly higher detection rates (91.5% vs. 83.1%) and total coincidence with clinical diagnoses (73.8% vs. 63.9%) [1] [29].
For blood samples from sepsis patients, gDNA-based mNGS (equivalent to wcDNA) with host depletion filtration detected all expected pathogens with an average of 9,351 microbial reads per million (RPM), over tenfold higher than cfDNA-based methods (95-1,488 RPM) [27] [9].
Pathogen-Type Detection Capabilities
The performance of each method varies significantly depending on the type of pathogen targeted, reflecting biological differences in pathogen localization and DNA release.
Table 3: Pathogen-Type Detection Performance
| Pathogen Type | wcDNA mNGS Performance | cfDNA mNGS Performance | Key Findings |
|---|---|---|---|
| Fungi | Detected 45/60 species in BALF [1] | Detected 60/60 species in BALF; 31.8% exclusively by cfDNA [1] | cfDNA superior for low-load fungi |
| Viruses | Detected 43/53 species in BALF [1] | Detected 53/53 species in BALF; 38.6% exclusively by cfDNA [1] | cfDNA superior for viral detection |
| Intracellular Bacteria | Limited detection for some species [1] | 26.7% detected exclusively by cfDNA in BALF [1] | cfDNA better for intracellular microbes |
| General Bacteria | 70.7% consistency with culture in body fluids [2] | Lower consistency vs. culture (46.67%) [2] | wcDNA superior for standard bacterial detection |
In BALF samples, cfDNA mNGS demonstrated particular advantages for detecting fungi (31.8% detected exclusively by cfDNA), viruses (38.6% exclusive to cfDNA), and intracellular microbes (26.7% exclusive to cfDNA) [1]. These patterns suggest cfDNA may be more effective for pathogens that reside intracellularly or release DNA fragments into biofluids.
Impact of Host DNA and Sequencing Depth
The proportion of host DNA in a sample directly impacts the sequencing depth required for adequate microbial genome coverage. Research shows that as host DNA percentage increases, sensitivity for detecting low-abundance microorganisms decreases significantly, particularly when sequencing depth is compromised [26]. Samples with 90% host DNA require substantially deeper sequencing to achieve comparable sensitivity to samples with lower host DNA content [26].
Host depletion techniques applied to wcDNA samples can dramatically improve microbial recovery. One study utilizing a Zwitterionic Interface Ultra-Self-assemble Coating (ZISC)-based filtration device achieved >99% white blood cell removal, reducing host DNA background and increasing microbial reads from 925 RPM to 9,351 RPM in clinical blood samples - a tenfold enrichment [27]. This approach significantly enhanced the sensitivity of gDNA-based mNGS, enabling 100% detection of pathogens in culture-positive sepsis samples [27].
Experimental Protocols and Methodologies
Standardized Workflows for wcDNA and cfDNA mNGS
The methodological differences between wcDNA and cfDNA mNGS begin at the sample processing stage and extend through library preparation:
cfDNA mNGS Protocol:
- Sample Processing: Centrifuge clinical sample (e.g., BALF, blood) at 20,000 × g for 15 minutes [2]
- DNA Extraction: Extract cfDNA from 400 μL supernatant using specialized kits (e.g., VAHTS Free-Circulating DNA Maxi Kit) [2]
- Library Preparation: Use ultra-low input library prep kits (e.g., QIAseq Ultralow Input Library Kit) [1] [29]
- Sequencing: Sequence on platforms such as Illumina NextSeq 550 or NovaSeq with ~26 million reads per sample [2]
wcDNA mNGS Protocol:
- Sample Processing: Retain precipitate after centrifugation; add beating beads for mechanical lysis [2]
- Optional Host Depletion: Apply filtration (e.g., ZISC-based filter) or other depletion methods [27]
- DNA Extraction: Extract wcDNA from precipitate using standard kits (e.g., Qiagen DNA Mini Kit) [2]
- Library Preparation: Prepare libraries using standard DNA library prep kits (e.g., VAHTS Universal Pro DNA Library Prep Kit) [2]
- Sequencing: Sequence on platforms such as Illumina NovaSeq with ~26 million reads per sample [2]
Host Depletion Techniques
For wcDNA mNGS, various host depletion strategies can significantly improve microbial signal:
- Filtration-based methods: Novel devices like the ZISC-based filter physically remove host cells while allowing microbes to pass through, achieving >99% white blood cell depletion [27]
- Differential lysis: Kits such as the QIAamp DNA Microbiome Kit selectively lyse human cells before microbial cell lysis [27]
- Methylation-based depletion: Techniques like the NEBNext Microbiome DNA Enrichment Kit target CpG-methylated host DNA for removal [27]
These methods reduce host DNA background from >95% to more manageable levels, dramatically increasing microbial read counts and improving detection sensitivity for low-abundance pathogens [27] [9].
Research Reagent Solutions
Successful implementation of wcDNA and cfDNA mNGS requires specific reagent systems optimized for different sample types and applications.
Table 4: Essential Research Reagents for mNGS Studies
| Reagent Category | Specific Product Examples | Application & Function |
|---|---|---|
| cfDNA Extraction Kits | VAHTS Free-Circulating DNA Maxi Kit (Vazyme) [2] | Extracts short DNA fragments from supernatant/plasma |
| wcDNA Extraction Kits | Qiagen DNA Mini Kit [2] | Extracts genomic DNA from cell pellets |
| Ultra-Low Input Library Prep | QIAseq Ultralow Input Library Kit (QIAGEN) [1] [29] | Constructs sequencing libraries from minimal DNA input |
| Standard DNA Library Prep | VAHTS Universal Pro DNA Library Prep Kit (Vazyme) [2] | Prepares sequencing libraries from sufficient DNA inputs |
| Host Depletion Filters | ZISC-based filtration device (Micronbrane) [27] | Physically removes host cells from whole blood samples |
| Differential Lysis Kits | QIAamp DNA Microbiome Kit (Qiagen) [27] | Selectively lyses human cells before microbial lysis |
| Methylation-Based Depletion | NEBNext Microbiome DNA Enrichment Kit (NEB) [27] | Removes CpG-methylated host DNA via magnetic beads |
Integrated Analysis and Future Directions
The comparative data reveals that neither wcDNA nor cfDNA mNGS is universally superior; instead, they offer complementary strengths. wcDNA mNGS, particularly when coupled with effective host depletion strategies, demonstrates excellent performance for bacterial detection in body fluids and blood [2] [27]. Conversely, cfDNA mNGS shows distinct advantages for detecting viruses, fungi, and intracellular pathogens in respiratory samples [1] [29].
This synergy suggests that a combined approach may optimize diagnostic yield. One clinical study evaluating both methods in parallel found that integrating cfDNA and cellular DNA mNGS results achieved higher diagnostic efficacy (ROC AUC: 0.8583) than either method alone (cfDNA AUC: 0.8041; cellular DNA AUC: 0.7545) [28].
Future methodological developments will likely focus on enhancing host depletion efficiency for wcDNA protocols and improving sensitivity for low-abundance mcfDNA in cfDNA approaches. Additionally, standardized bioinformatics pipelines and reporting criteria are needed to ensure consistent interpretation across laboratories and sample types [2] [30]. As sequencing costs continue to decline and methodologies refine, dual-mode mNGS testing may become increasingly feasible for challenging diagnostic scenarios where conventional methods have failed.
Strategic Application: Selecting wcDNA or cfDNA mNGS for Different Clinical Specimens and Pathogens
Metagenomic next-generation sequencing (mNGS) has revolutionized pathogen detection by enabling unbiased identification of microorganisms without prior knowledge of the causative agent. Within this field, a critical methodological consideration is the choice between whole-cell DNA (wcDNA) and cell-free DNA (cfDNA) approaches for optimal diagnostic yield. wcDNA mNGS targets intact microbial cells and intracellular pathogens through DNA extraction from pelleted samples or tissue homogenates, whereas cfDNA mNGS sequences extracellular DNA released from lysed cells into body fluids. Understanding the performance characteristics, limitations, and optimal applications of wcDNA mNGS is essential for researchers and clinicians seeking to implement this technology effectively in infectious disease diagnostics. This guide synthesizes current evidence to objectively compare wcDNA and cfDNA mNGS approaches, with particular emphasis on sample type selection to maximize detection sensitivity and specificity across diverse clinical scenarios.
Performance Comparison: wcDNA vs. cfDNA mNGS
Recent comparative studies reveal distinct performance profiles for wcDNA and cfDNA mNGS across different sample types and pathogen categories. The table below summarizes key performance metrics from clinical evaluations:
Table 1: Overall diagnostic performance of wcDNA vs. cfDNA mNGS
| Performance Metric | wcDNA mNGS | cfDNA mNGS | Combined Approach | Study Details |
|---|---|---|---|---|
| Sensitivity | 74.07% | Not reported | Higher than individual methods | Body fluids (n=125) [2] |
| Specificity | 56.34% | Not reported | Not reported | Body fluids (n=125) [2] |
| Concordance with culture | 63.33%-70.7% | 46.67% | Not reported | Body fluids (n=30-41) [2] |
| Detection rate | 83.1% | 91.5% | Not reported | BALF (n=130) [1] |
| ROC AUC | 0.7545 | 0.8041 | 0.8583 | Body fluids (n=248) [31] [28] |
| Limit of Detection | 27-466 CFU/mL | 9.3-149 GE/mL | Not reported | Laboratory validation [31] |
Performance by Pathogen Type
The effectiveness of wcDNA and cfDNA mNGS varies significantly depending on the microbial category:
Table 2: Performance comparison by pathogen type
| Pathogen Category | wcDNA mNGS Advantages | cfDNA mNGS Advantages | Clinical Context |
|---|---|---|---|
| Bacteria | Superior detection in high-host background samples [31] | Lower host DNA proportion improves detection sensitivity | Abdominal infections, sterile body fluids [2] [31] |
| Fungi | 19.7% exclusively detected | 31.8% exclusively detected | Pulmonary infections [1] |
| Viruses | Limited detection capability | Excellent detection (ROC AUC: 0.9814 in blood) [31] | Bloodstream infections [31] |
| Intracellular Microbes | 6.7% exclusively detected | 26.7% exclusively detected | Pulmonary infections [1] |
Performance by Sample Type
The optimal choice between wcDNA and cfDNA mNGS is heavily influenced by the sample matrix being tested:
Table 3: Performance across sample types
| Sample Type | Recommended Method | Rationale | Study Evidence |
|---|---|---|---|
| Bronchoalveolar Lavage Fluid (BALF) | cfDNA preferred | Higher detection rate (91.5% vs 83.1%) and total coincidence rate (73.8% vs 63.9%) | Pulmonary infections (n=130) [1] |
| High Host-Background Samples | wcDNA superior | Better performance in samples with abundant human DNA | Body fluids [31] |
| Blood | cfDNA superior | Optimal for viral detection (ROC AUC: 0.9814) | Multicenter evaluation [31] |
| Sterile Body Fluids | Combined approach | Maximizes diagnostic efficacy | Pleural, pancreatic, ascites, CSF (n=248) [31] |
Experimental Protocols and Methodologies
Standardized wcDNA mNGS Workflow
The following workflow diagram illustrates the core experimental procedures for wcDNA mNGS:
Figure 1: Standardized workflow for wcDNA mNGS testing
Detailed Methodological Protocols
Sample Processing and DNA Extraction
For body fluid samples (pleural fluid, ascites, BALF, CSF), the standardized protocol involves:
- Centrifugation: 20,000 × g for 15 minutes to separate cellular components from supernatant [2]
- Cell Lysis: Addition of nickel beads (3-mm) to retained precipitate, shaken at 3,000 rpm for 5 minutes [2]
- DNA Extraction: Using commercial kits (Qiagen DNA Mini Kit) following manufacturer's protocol [2]
- DNA Quantification: Fluorometric methods (Qubit 4.0) for accurate quantification prior to library preparation [1]
Library Preparation and Sequencing
- Library Construction: VAHTS Universal Pro DNA Library Prep Kit for Illumina [2]
- Sequencing Platform: Illumina NovaSeq with 2×150 paired-end configuration [2]
- Sequencing Depth: Approximately 8 GB of data per sample (≈26.7 million reads) [2]
- Controls: Negative controls (sterile deionized water) and positive controls with each batch [1]
Bioinformatic Analysis
- Quality Control: Removal of adapter sequences, low-quality, and short reads (<35bp) [1]
- Host DNA Depletion: Mapping to human reference genome (hg38) using bowtie2 [1]
- Pathogen Identification: Alignment against comprehensive microbial genome databases [1]
- Validation: Comparison with culture results, 16S/ITS amplicon sequencing, or qPCR [31]
Technical Considerations and Optimization Strategies
Decision Framework for Method Selection
The choice between wcDNA and cfDNA mNGS depends on multiple experimental and clinical factors:
Figure 2: Decision framework for selecting between wcDNA and cfDNA mNGS
The Scientist's Toolkit: Essential Research Reagents
Table 4: Essential research reagents for wcDNA mNGS workflows
| Reagent/Kits | Manufacturer | Specific Function | Application Context |
|---|---|---|---|
| Qiagen DNA Mini Kit | Qiagen | wcDNA extraction from cell pellets | Body fluids, tissue specimens [2] |
| VAHTS Universal Pro DNA Library Prep Kit | Vazyme Biotech | NGS library preparation | Low-input DNA samples [2] |
| QIAseq Ultralow Input Library Kit | QIAGEN | Library preparation for limited DNA | Single-cell or low biomass samples [1] |
| gentleMACS Dissociator | Miltenyi Biotec | Tissue dissociation for single-cell suspension | Tissue specimens [32] |
| PythoN Tissue Dissociation System | Singleron | Integrated tissue dissociation | Multiple tissue types (200+ validated) [32] |
| Singulator Platform | S2 Genomics | Automated cell/nuclei isolation | Fresh, frozen, and FFPE tissues [32] |
Discussion and Clinical Implications
Integrated Interpretation of Findings
The comparative data presented reveals that neither wcDNA nor cfDNA mNGS universally outperforms the other across all clinical scenarios. Instead, these methods exhibit complementary strengths that can be strategically leveraged based on clinical context, suspected pathogen category, and sample type availability. wcDNA mNGS demonstrates particular value in scenarios involving high host-background samples and bacterial infections, where intact microbial cells are likely to be present in sufficient quantities for detection [2] [31]. The higher specificity of wcDNA mNGS for bacterial pathogens in body fluids makes it particularly valuable for abdominal infections and other non-bloodstream infections where intracellular pathogens may be present.
Conversely, cfDNA mNGS excels in detecting viral pathogens and intracellular microorganisms that may be released into the extracellular space through cell lysis or active secretion [31] [1]. The superior performance of cfDNA mNGS in blood samples aligns with the natural distribution of cell-free microbial DNA in circulation, making it the method of choice for bloodstream infections and systemic viral infections.
Limitations and Technical Challenges
Despite its advantages, wcDNA mNGS presents several technical challenges that require consideration:
- Lower sensitivity for viruses and intracellular pathogens compared to cfDNA approaches [1]
- Variable performance across different sample types and pathogen categories [2] [31]
- Compromised specificity (56.34%) in some clinical evaluations, necessitating careful result interpretation [2]
- Dependence on sample processing protocols that preserve cellular integrity [32]
Future Directions and Clinical Applications
The emerging consensus from recent studies supports a combined approach utilizing both wcDNA and cfDNA mNGS when feasible, as this strategy achieves the highest diagnostic efficacy (ROC AUC: 0.8583) compared to either method alone [31] [28]. For resource-limited settings or when sample volume is constrained, the decision framework provided in this guide offers evidence-based guidance for method selection.
Future research directions should focus on standardizing extraction protocols, establishing validated cutoff values for pathogen identification, and developing integrated bioinformatic pipelines that can simultaneously analyze both wcDNA and cfDNA sequencing data. Additionally, more comprehensive cost-benefit analyses are needed to guide the implementation of these technologies in routine clinical practice.
For clinical researchers and diagnostic developers, these findings underscore the importance of aligning methodological approaches with clinical questions and sample characteristics rather than seeking a universal solution for pathogen detection across all scenarios.
Metagenomic next-generation sequencing (mNGS) has revolutionized pathogen detection by enabling unbiased identification of microorganisms in clinical samples. Two primary approaches have emerged for nucleic acid extraction: whole-cell DNA (wcDNA) sequencing, which targets genomic DNA from intact microorganisms, and cell-free DNA (cfDNA) sequencing, which targets microbial DNA fragments circulating in body fluids. The optimal specimen type and processing method vary significantly depending on the clinical context, pathogen characteristics, and infection site. This guide objectively compares the performance of cfDNA mNGS across three key sample types—plasma, cerebrospinal fluid (CSF), and bronchoalveolar lavage fluid (BALF) supernatant—within the broader framework of comparing wcDNA versus cfDNA methodologies for pathogen identification, providing researchers with evidence-based selection criteria.
Performance Comparison Across Sample Types
Analytical and Diagnostic Performance Metrics
Table 1: Performance characteristics of cfDNA mNGS across different sample types
| Sample Type | Primary Applications | Key Advantages | Limitations | Reported Sensitivity | Reported Specificity |
|---|---|---|---|---|---|
| Plasma | Bloodstream infections, disseminated infections, immunocompromised hosts | Minimally invasive, ideal for detecting circulating pathogen DNA, reflects disseminated infection | Lower pathogen DNA concentration, susceptible to background human DNA interference | 76.44%-77.70% (BSI diagnosis) [33] | Higher for viral detection (AUC: 0.9814) [31] |
| CSF | Central nervous system infections, meningitis, encephalitis | Low host background, high clinical relevance for CNS pathogens | Invasive collection procedure, limited volume typically obtained | Associated with disease progression/metastasis in MB [34] | Specificity not explicitly quantified in available studies |
| BALF Supernatant | Pulmonary infections, pneumonia, fungal detection | Higher fungal/viral detection vs. wcDNA, better performance for intracellular pathogens | Potential contamination from colonizing microbes in respiratory tract | 91.5% detection rate [29] | Improved RPM values for Aspergillus detection [21] |
Quantitative Pathogen Detection Metrics
Table 2: Comparison of quantitative detection capabilities across sample types
| Sample Type | Optimal Pathogen Targets | Superiority Over wcDNA mNGS | Read Thresholds | Limits of Detection |
|---|---|---|---|---|
| Plasma | Viruses, disseminated bacterial/fungal infections | Comparable accuracy to mNGS at reduced cost (tNGS) [33] | RPM ≥6 for common bacteria; ≥0.5 for fungi/mycobacteria [33] | 9.3-149 GE/mL [31] |
| CSF | CNS pathogens, particularly in high-grade infections | Shorter fragment size (150-200bp) indicates true cfDNA [34] | Not explicitly stated in studies | Not quantified in pathogen detection context |
| BALF Supernatant | Fungi (31.8%), viruses (38.6%), intracellular microbes (26.7%) [29] | Higher RPM for Aspergillus (cut-off >4.5 predicts true PA) [21] | Standard mNGS thresholds apply | Not explicitly determined |
Experimental Protocols and Methodologies
Standardized cfDNA Extraction and Analysis Workflow
The following diagram illustrates the core experimental workflow for cfDNA mNGS that is commonly adapted across different sample types:
Diagram 1: Core cfDNA mNGS workflow. This generalized protocol is adapted specifically for plasma, CSF, and BALF supernatant samples with modifications at key steps.
Sample-Specific Processing Protocols
Plasma Processing for Bloodstream Infections
For plasma cfDNA analysis, blood samples are collected in anticoagulant tubes and processed following a standardized protocol [33] [35]. Samples are centrifuged at 1900 × g at 4°C for 10 minutes to separate cellular components. The resulting supernatant (plasma) is transferred to a fresh tube and subjected to a second centrifugation at 16,000 × g for 10 minutes to remove any remaining cellular debris. cfDNA is extracted from 0.5-1 mL of plasma using specialized kits (QIAamp Circulating Nucleic Acid Kit or PathoXtract Plasma Nucleic Acid Kit) according to manufacturers' protocols [33] [34]. The extracted cfDNA undergoes library preparation using kits such as the KAPA DNA HyperPrep Kit or QIAseq Ultralow Input Library Kit, followed by sequencing on platforms like Illumina NextSeq 550 or MGISEQ-2000 [29] [33] [35].
CSF Processing for CNS Infections
CSF samples collected via lumbar puncture or during surgical procedures are processed with particular attention to potential low biomass [34]. Fresh CSF is centrifuged at 4°C (1400 × g for 5 minutes) within 2-3 hours of collection. The supernatant is carefully transferred to cryotubes and stored at -80°C until processing. cfDNA extraction employs the QIAamp Circulating Nucleic Acid Kit, with critical verification of fragment size distribution (150-200 bp) using Agilent 2100 Bioanalyzer to confirm true cfDNA rather than cellular genomic DNA [34]. Library preparation typically requires amplification kits designed for low input DNA, such as the KAPA Library Amplification Kit, with targeted capture approaches sometimes employed to enhance sensitivity for CNS pathogens.
BALF Supernatant Processing for Pulmonary Infections
BALF samples are centrifuged at varying forces (12,075 × g for 5 minutes to 20,000 × g for 15 minutes) to separate supernatant from cellular components [36] [31] [21]. The supernatant is carefully collected for cfDNA extraction using the QIAamp DNA Micro Kit or similar systems. For comprehensive pathogen detection, simultaneous RNA extraction may be performed for RNA viruses, followed by reverse transcription to cDNA [35]. Library preparation utilizes kits such as the QIAseq Ultralow Input Library Kit or VAHTS Universal Pro DNA Library Prep Kit, with sequencing typically on Illumina platforms (NextSeq 550, NovaSeq) [29] [21].
Complementary Value of cfDNA and wcDNA mNGS
Integrated Testing Approach
The relationship between cfDNA and wcDNA mNGS testing is complementary rather than competitive, as illustrated in the following decision pathway:
Diagram 2: Decision pathway for sample type selection. This flowchart guides appropriate sample selection based on clinical presentation and demonstrates the complementary relationship between cfDNA and wcDNA testing approaches.
Performance Synergy
Research demonstrates that combining cfDNA and wcDNA mNGS achieves superior diagnostic efficacy compared to either method alone. A comprehensive evaluation of 248 specimens showed the area under the ROC curve increased to 0.8583 for combined testing, compared to 0.8041 for cfDNA alone and 0.7545 for cellular DNA alone [31] [28]. In pulmonary aspergillosis, combining BALF-cfDNA mNGS with conventional tests significantly improved sensitivity (89.47% vs. 47.37%) and ROC analysis (0.813 vs. 0.66) compared to conventional tests alone [21]. For pneumonia-derived sepsis, simultaneous plasma and BALF mNGS testing identified definite causative pathogens in 55.6% of cases, substantially higher than either sample type alone (20.8% for plasma, 18.8% for BALF) [35].
Essential Research Reagent Solutions
Table 3: Key reagents and kits for cfDNA mNGS research
| Reagent/Kits | Specific Examples | Application Function | Sample Type Compatibility |
|---|---|---|---|
| cfDNA Extraction Kits | QIAamp Circulating Nucleic Acid Kit, PathoXtract Plasma Nucleic Acid Kit, VAHTS Free-Circulating DNA Maxi Kit | Isolation of short-fragment cfDNA from body fluids while removing cellular genomic DNA | Plasma, CSF, BALF supernatant |
| Library Preparation Kits | QIAseq Ultralow Input Library Kit, KAPA DNA HyperPrep Kit, VAHTS Universal Pro DNA Library Prep Kit | Construction of sequencing libraries from low-input cfDNA samples | Universal across sample types |
| Nucleic Acid Quantification | Qubit Fluorometer with dsDNA HS Assay, Agilent 2100 Bioanalyzer | Accurate quantification and quality assessment of low-concentration cfDNA | Universal across sample types |
| Host DNA Depletion Reagents | Custom probes for human genome sequences | Reduction of host background to improve microbial signal detection | Plasma (high host background) |
| Target Enrichment Systems | Ultra-broad hybrid capture panels (e.g., 1872 pathogen panel) | Enhanced detection of low-abundance pathogens through probe-based enrichment | Plasma (tNGS applications) |
The selection of optimal sample types for cfDNA mNGS depends on the clinical scenario, target pathogens, and analytical priorities. Plasma cfDNA excels for bloodstream and disseminated infections, particularly in immunocompromised hosts, and shows special utility for viral detection. BALF supernatant cfDNA demonstrates superior performance for respiratory fungi, viruses, and intracellular pathogens compared to wcDNA approaches. CSF cfDNA offers unique value in neuro-infections and is strongly associated with disease progression in central nervous system pathologies. Rather than considering these approaches in isolation, researchers should recognize the complementary value of cfDNA and wcDNA mNGS, as their combined application consistently demonstrates enhanced diagnostic efficacy across multiple sample types and clinical scenarios.
Superiority of cfDNA for Detecting Viruses, Fungi, and Intracellular Pathogens
Metagenomic next-generation sequencing (mNGS) has revolutionized pathogen detection by enabling unbiased, comprehensive analysis of microbial nucleic acids in clinical samples. Two primary approaches have emerged for sample processing: whole-cell DNA (wcDNA) mNGS, which sequences DNA from intact microbial cells, and cell-free DNA (cfDNA) mNGS, which targets freely circulating microbial DNA fragments. This guide objectively compares the performance of these methods, with a specific focus on the demonstrated superiority of cfDNA mNGS for detecting viruses, fungi, and intracellular pathogens. Understanding the technical basis for these performance differences is critical for researchers and clinicians to select the optimal method for specific diagnostic and research applications.
Fundamental Technical Differences Between cfDNA and wcDNA mNGS
The divergent performance characteristics of wcDNA and cfDNA mNGS stem from fundamental differences in their source materials and processing workflows.
Whole-cell DNA mNGS begins with a sample processing step designed to lyse intact microbial cells—including bacteria, fungi, and parasites—to release their genomic DNA. This process often involves mechanical disruption (e.g., bead-beating) and enzymatic digestion to break down rigid cell walls. The extracted DNA represents the collective genomic content of viable microorganisms present in the sample at the time of collection [2] [9].
In contrast, cell-free DNA mNGS analyzes extracellular DNA fragments circulating in biofluids. These fragments are typically short (150-200 base pairs) and are derived from various biological processes, including cellular apoptosis, necrosis, and active release from pathogens. For microbial detection, cfDNA mNGS specifically targets microbial cell-free DNA (mcfDNA) that is released into host body fluids during infection [37] [9].
The following diagram illustrates the key procedural differences between these two approaches:
Table 1: Core Technical Distinctions Between cfDNA and wcDNA mNGS
| Characteristic | cfDNA mNGS | wcDNA mNGS |
|---|---|---|
| Source Material | Cell-free DNA in supernatant | Genomic DNA from intact microbial cells |
| Extraction Process | From plasma/supernatant after centrifugation | Direct from sample or cell pellet |
| Typical Fragment Size | 150-200 bp (short fragments) | Varies (longer fragments) |
| Primary Origin | Apoptosis, necrosis, active release | Viable microorganisms |
| Host DNA Interference | High (≥95% host DNA in blood) [2] | Variable (often lower than cfDNA) |
| Best Suited For | Viruses, fungi, intracellular pathogens, difficult-to-lyse organisms | Routine bacterial detection, extracellular pathogens |
Comparative Performance Data for Different Pathogen Classes
Detection of Viral Pathogens
cfDNA mNGS demonstrates particular advantages in viral detection. In a comprehensive study of pulmonary infections using bronchoalveolar lavage fluid (BALF) samples, cfDNA mNGS detected 38.6% more viruses than wcDNA mNGS (27/70 vs. 10/70) [1]. This enhanced detection capability stems from the natural biology of viral infections, where viral DNA is often present in cell-free form due to viral lysis and replication cycles.
The superiority of cfDNA for viral detection is further supported by its higher sensitivity for viruses with low abundance in clinical samples. Researchers observed that cfDNA mNGS consistently identified more viral reads per million (RPM) for low-load viruses compared to wcDNA mNGS, making it particularly valuable for detecting subclinical or early-stage viral infections [1].
Detection of Fungal Pathogens
Fungal pathogens present unique challenges for mNGS detection due to their rigid cell walls, which can resist standard lysis procedures used in wcDNA extraction. Comparative studies show cfDNA mNGS detected 31.8% more fungi than wcDNA mNGS (21/66 vs. 13/66) in BALF samples from patients with pulmonary infections [1].
This performance advantage is particularly relevant for invasive fungal infections (IFIs), where timely diagnosis is critical for patient outcomes. A systematic review and meta-analysis found that cfDNA positivity was observed in 79% of patients with proven fungal infections (95% CI: 0.62–0.90), supporting its value as a minimally invasive, culture-independent diagnostic marker [37].
Detection of Intracellular Pathogens
Intracellular pathogens, including bacteria like Mycobacterium tuberculosis and viruses, are frequently better detected by cfDNA mNGS. Research demonstrates cfDNA mNGS identified 26.7% more intracellular microbes than wcDNA mNGS (8/30 vs. 2/30) [1]. This enhanced detection occurs because intracellular pathogens release their genetic material into the circulation during infection, making it accessible to cfDNA testing without requiring complex lysis procedures to liberate DNA from within host cells.
The following table summarizes key performance metrics from comparative studies:
Table 2: Comprehensive Performance Comparison of cfDNA vs. wcDNA mNGS
| Performance Metric | cfDNA mNGS | wcDNA mNGS | Study Details |
|---|---|---|---|
| Pathogen Detection Rate | 91.5% | 83.1% | BALF samples from 130 patients with pulmonary infections [1] |
| Total Coincidence Rate | 73.8% | 63.9% | Compared to composite reference standard [1] |
| Fungal Detection | 31.8% more fungi detected | Baseline | BALF samples [1] |
| Viral Detection | 38.6% more viruses detected | Baseline | BALF samples [1] |
| Intracellular Microbe Detection | 26.7% more intracellular pathogens | Baseline | BALF samples [1] |
| Concordance with Culture | 46.67% (14/30) | 63.33% (19/30) | Body fluid samples [2] |
| Mean Host DNA Proportion | 95% | 84% | Body fluid samples (p < 0.05) [2] |
| Analytical Sensitivity (Sepsis) | Inconsistent sensitivity | 100% detection with host depletion | Blood culture-positive samples [27] |
Detailed Experimental Protocols for Performance Validation
Sample Processing and DNA Extraction
cfDNA Extraction Protocol:
- Sample Collection: Collect blood samples in Cell-Free DNA BCT tubes (Streck) or K2EDTA tubes [38].
- Plasma Separation: Perform two consecutive centrifugation steps - first at 400×g for 15 minutes to separate plasma from blood cells, followed by 16,000×g for 10 minutes to remove residual cells and debris [1] [27].
- cfDNA Extraction: Extract cfDNA from 400 μL to 5.5 mL of plasma using the MagMax Cell-Free Total Nucleic Acid Isolation Kit (Thermo Fisher Scientific) or VAHTS Free-Circulating DNA Maxi Kit (Vazyme Biotech) according to manufacturers' instructions [2] [38].
- DNA Quantification: Assess cfDNA quantity using dsDNA HS assay kit on Qubit Fluorometer and quality with Agilent High Sensitivity D1000 ScreenTape System [38].
wcDNA Extraction Protocol:
- Sample Processing: For body fluids, centrifuge at 20,000×g for 15 minutes and retain the precipitate [2].
- Cell Lysis: Add nickel beads to the precipitate and shake at 3,000 rpm for 5 minutes for mechanical disruption of microbial cells [2].
- DNA Extraction: Extract wcDNA using the Qiagen DNA Mini Kit according to manufacturer's protocol [2].
- DNA Assessment: Quantify DNA and check quality using spectrophotometric or fluorometric methods.
Library Preparation and Sequencing
Library Construction:
- Fragment Size Selection: For cfDNA, target fragment sizes of ~180 bp are typical, while wcDNA fragments are typically larger (~300 bp) [39] [38].
- Adapter Ligation: Use the VAHTS Universal Pro DNA Library Prep Kit for Illumina (Vazyme Biotech) or similar commercial kits to attach sequencing adapters [2].
- Library Amplification: Perform PCR amplification with cycle optimization based on input DNA quantity and quality.
- Library Quality Control: Assess library concentration by qPCR using the Ion Universal Quantitation Kit and fragment size distribution [38].
Sequencing Parameters:
- Platform: Illumina NovaSeq or similar high-throughput sequencer
- Configuration: 2×150 bp or 2×250 bp paired-end sequencing
- Read Depth: Minimum 10 million reads per sample, typically 8-20 GB data per sample [2] [27]
Bioinformatic Analysis
Data Processing Pipeline:
- Quality Control: Remove adapter sequences and low-quality reads using tools like Trimmomatic or Cutadapt.
- Host DNA Depletion: Map reads to human reference genome (hg38) using Bowtie2 or BWA and remove aligned reads [2] [1].
- Microbial Identification: Align non-host reads to comprehensive microbial databases using BLAST or similar tools.
- Pathogen Reporting: Apply criteria for valid pathogen identification: z-score >3 compared to negative controls, reads mapping to multiple genomic regions, and minimum read counts (typically >100 for bacteria, >10 for fungi/viruses) [2].
Conceptual Framework for cfDNA Superiority with Specific Pathogens
The following diagram illustrates the biological mechanisms underlying cfDNA mNGS's enhanced performance with challenging pathogens:
The superior performance of cfDNA mNGS for viruses, fungi, and intracellular pathogens can be attributed to several interconnected biological and technical factors:
Elimination of Lysis Barriers: Fungal cell walls (chitin) and viral capsids can resist standard lysis methods, leading to under-representation in wcDNA mNGS. cfDNA bypasses this requirement entirely [1] [9].
Access to Circulating Genetic Material: During active infection, pathogens release genetic material into biofluids through various mechanisms including apoptosis, necrosis, and active secretion. cfDNA directly captures this circulating genetic evidence of infection [37] [9].
Reduced Host Cell Interference: Intracellular pathogens sequestered within host cells require complex processing to liberate pathogen DNA. cfDNA represents genetic material already liberated from cellular compartments [1].
Superior Representation of Infection Burden: The quantity of microbial cfDNA correlates with active infection burden and dynamics, providing a more accurate representation of the current infection state compared to cellular genomic DNA [9].
Essential Research Reagents and Tools
Table 3: Essential Research Reagents for cfDNA and wcDNA mNGS Studies
| Category | Specific Products | Application Purpose | Key Considerations |
|---|---|---|---|
| Blood Collection Tubes | Cell-Free DNA BCT (Streck), K2EDTA tubes | Sample stabilization | BCT tubes stabilize nucleated cells and prevent background DNA release |
| cfDNA Extraction Kits | MagMax Cell-Free Total Nucleic Acid Isolation Kit, VAHTS Free-Circulating DNA Maxi Kit | Isolation of cell-free DNA | Optimized for low-concentration, fragmented DNA |
| wcDNA Extraction Kits | Qiagen DNA Mini Kit, ZymoBIOMICS DNA Miniprep Kit | Microbial DNA isolation | Include bead-beating step for comprehensive cell disruption |
| Library Prep Kits | VAHTS Universal Pro DNA Library Prep Kit, QIAseq Ultralow Input Library Kit | NGS library construction | Ultralow input kits essential for limited cfDNA samples |
| Host Depletion Kits | QIAamp DNA Microbiome Kit, NEBNext Microbiome DNA Enrichment Kit | Reduction of human background | Critical for wcDNA from high-host content samples |
| Sequencing Platforms | Illumina NovaSeq, NextSeq | High-throughput sequencing | Minimum 10M reads/sample recommended |
| Bioinformatic Tools | Bowtie2, BWA, Kraken2, Pavian | Data analysis | Specialized pipelines for microbial identification |
The accumulating evidence from comparative studies strongly supports the superiority of cfDNA mNGS for detecting specific pathogen categories, particularly viruses, fungi, and intracellular organisms. This advantage stems from fundamental biological and technical factors that enable cfDNA mNGS to overcome key limitations of traditional whole-cell DNA approaches. While wcDNA mNGS maintains value for certain applications, researchers and clinicians should consider cfDNA mNGS as the primary approach for diagnosing infections involving difficult-to-lyse or intracellular pathogens, and in cases where conventional testing has failed to identify causative organisms despite high clinical suspicion. The continued optimization of cfDNA extraction, sequencing, and bioinformatic analysis will further enhance its diagnostic utility across the spectrum of infectious diseases.
Enhanced Performance of wcDNA mNGS in Abdominal and Bacterial Infections
Metagenomic next-generation sequencing (mNGS) has emerged as a transformative, hypothesis-free tool for pathogen identification, capable of detecting a broad spectrum of microorganisms directly from clinical specimens [40]. A critical technical consideration in mNGS workflow is the choice of nucleic acid source: whole-cell DNA (wcDNA), which is extracted from intact microbial and host cells, or cell-free DNA (cfDNA), which is extracted from the supernatant after centrifugation and captures freely circulating microbial genetic material [29] [1]. While both methods are widely used, their performance characteristics differ significantly across clinical scenarios. This guide objectively compares their performance, with a specific focus on the demonstrated superiority of wcDNA mNGS in the context of abdominal and typical bacterial infections, providing researchers and drug development professionals with the experimental data and protocols necessary to inform their diagnostic strategies.
Performance Comparison: wcDNA mNGS vs. cfDNA mNGS
The optimal choice between wcDNA and cfDNA mNGS is highly context-dependent, influenced by the sample type, the suspected pathogen category, and the clinical syndrome. The following tables summarize key comparative data.
Table 1: Overall Diagnostic Performance in Different Sample Types
| Infection/Sample Type | Metric | wcDNA mNGS | cfDNA mNGS | Reference |
|---|---|---|---|---|
| Abdominal & Body Fluids | Concordance with Culture | 63.33% (19/30) | 46.67% (14/30) | [2] |
| Pulmonary (BALF) | Detection Rate | 83.1% | 91.5% | [29] [1] |
| Central Nervous System (CSF) | Sensitivity | 32.0% | 60.2% | [41] |
| Sepsis (Blood) | Sensitivity (Bacteria/Fungi) | 88% (bc-mNGS) | 100% (p-mNGS) | [42] |
Table 2: Pathogen-Class-Specific Detection Performance
| Pathogen Category | wcDNA mNGS Advantage | cfDNA mNGS Advantage | Key Context |
|---|---|---|---|
| Bacteria (Typical) | Demonstrates higher concordance with culture results in body fluids [2]. | -- | Particularly noted in abdominal infections. |
| Fungi | -- | Detects 31.8% more fungi with low microbial loads in BALF [29]. | Especially advantageous for detecting low-load fungi like Aspergillus [43]. |
| Viruses | -- | Detects 38.6% more viruses in BALF [29]. | Superior for viral CNS infections [41]. |
| Intracellular Bacteria | -- | Detects 26.7% more intracellular microbes (e.g., M. tuberculosis) [29] [41]. | cfDNA avoids lysis steps that may compromise delicate pathogens. |
Experimental Protocols and Workflows
A clear understanding of the distinct experimental protocols for wcDNA and cfDNA extraction is crucial for interpreting their performance differences.
Key Sample Processing Methodologies
The primary divergence in protocol occurs at the initial sample preparation stage [2] [1]:
- wcDNA Extraction: The clinical sample (e.g., BALF, body fluid) is processed directly, often involving a bead-beating step to mechanically lyse intact microbial cells and release genomic DNA. This method captures DNA from both viable and non-viable microorganisms within cells.
- cfDNA Extraction: The clinical sample is first centrifuged to remove intact cells (both host and microbial). The cell-free supernatant is then used for DNA extraction, which primarily targets short fragments of DNA released from pathogens due to cell death or active secretion.
Detailed Protocol from Comparative Studies
A 2025 study on body fluid samples provides a representative and detailed protocol [2]:
- Sample Collection: 125 clinical body fluid samples (pleural, pancreatic, drainage, ascites, and cerebrospinal fluid) were collected.
- Centrifugation: Samples were centrifuged at 20,000 × g for 15 minutes.
- cfDNA Extraction: DNA was extracted from 400 μL of supernatant using the VAHTS Free-Circulating DNA Maxi Kit (Vazyme Biotech), following the manufacturer's instructions.
- wcDNA Extraction: The retained precipitate was used for wcDNA extraction. Two 3-mm nickel beads were added, and the sample was shaken at 3,000 rpm for 5 minutes for cell lysis. DNA was then extracted using the Qiagen DNA Mini Kit.
- Library Preparation & Sequencing: Libraries for both methods were prepared with the VAHTS Universal Pro DNA Library Prep Kit and sequenced on the Illumina NovaSeq platform with a 2 × 150 paired-end configuration, generating approximately 8 GB of data per sample.
The following diagram illustrates the core divergence in the sample processing workflows for wcDNA and cfDNA mNGS.
Mechanistic Insights and Analytical Considerations
The observed performance differences are not arbitrary but stem from fundamental biological and technical factors.
Host DNA Background
A significant challenge in mNGS is the high background of human host DNA, which can obscure microbial signals. The cfDNA fraction from body fluids was found to have a mean host DNA proportion of 95%, significantly higher than the 84% found in the wcDNA fraction [2]. This excessive host background in cfDNA can lower the sensitivity for detecting bacterial pathogens, particularly in abdominal infections where high microbial biomass is often expected.
Pathogen Viability and Clinical Relevance
The higher concordance of wcDNA mNGS with culture results—a traditional marker for viable pathogens—suggests it may better detect intact, viable microorganisms [2]. This is corroborated by co-metagenomic sequencing in sepsis, where bc-mNGS (blood-cell mNGS, analogous to wcDNA) showed higher agreement with blood culture than plasma cfDNA mNGS (p-mNGS) [42]. This makes wcDNA a compelling target for detecting active bacterial infections.
Diagnostic Decision Pathway
Integrating these findings into a diagnostic strategy requires a structured approach. The following diagram outlines a decision pathway for selecting between wcDNA and cfDNA mNGS based on clinical presentation.
The Scientist's Toolkit: Essential Research Reagents
The following table details key reagents and kits used in the featured comparative studies, which are essential for researchers aiming to establish or validate these mNGS protocols.
Table 3: Key Research Reagent Solutions for mNGS Workflows
| Reagent / Kit | Function in Protocol | Application Context |
|---|---|---|
| QIAamp DNA Micro Kit (QIAGEN) | Extraction of both cfDNA and wcDNA from low-volume samples like BALF and CSF [29] [41]. | Core extraction method in multiple pulmonary and CNS infection studies. |
| VAHTS Free-Circulating DNA Maxi Kit (Vazyme) | Specialized extraction of cell-free DNA from plasma or body fluid supernatant [2]. | Used in body fluid cfDNA studies for optimal yield of short-fragment DNA. |
| Qiagen DNA Mini Kit | Extraction of whole-cell DNA from cellular precipitates after lysis [2]. | Employed for wcDNA from body fluid samples, following bead-beating lysis. |
| VAHTS Universal Pro DNA Library Prep Kit (Vazyme) | Preparation of sequencing-ready libraries from extracted DNA [2]. | Used for library construction for both wcDNA and cfDNA in body fluid analysis. |
| QIAseq Ultralow Input Library Kit (QIAGEN) | Library construction from very low input DNA, suitable for cfDNA [29] [44]. | Applied in studies on BALF-cfDNA and plasma cfDNA where DNA input is limited. |
The comparative data clearly indicate that wcDNA mNGS demonstrates enhanced performance for pathogen identification in abdominal infections and other body fluids, particularly for typical bacterial pathogens, as evidenced by its higher concordance with culture results. This is likely due to its more effective capture of DNA from viable, intact microorganisms and a lower relative host DNA background in these sample types. Conversely, cfDNA mNGS excels in scenarios involving low pathogen loads, intracellular bacteria, viruses, and fungi, as seen in pulmonary and central nervous system infections. Therefore, the choice between wcDNA and cfDNA mNGS is not one of superiority but of appropriateness. Researchers and clinicians should base their selection on the clinical syndrome, sample type, and the specific pathogens under suspicion. A dual-protocol approach, or the use of co-metagenomic sequencing as explored in sepsis [42], may provide the most comprehensive diagnostic insight in complex cases.
The precise and timely identification of pathogens is a cornerstone of effective clinical management for serious infectious diseases, including central nervous system (CNS) infections, sepsis, and pulmonary aspergillosis. Metagenomic next-generation sequencing (mNGS) has emerged as a powerful, hypothesis-free tool for pathogen detection. This technology can be applied to two distinct types of nucleic acid templates: whole-cell DNA (wcDNA), which involves extracting total DNA from a clinical sample, and cell-free DNA (cfDNA), which targets microbial DNA fragments circulating in body fluids. This guide objectively compares the performance of wcDNA and cfDNA mNGS across three critical clinical scenarios, providing researchers and drug development professionals with consolidated experimental data and methodologies to inform their work.
Comparative Performance Data Across Clinical Case Studies
The following tables summarize key quantitative findings from recent studies comparing wcDNA-mNGS and cfDNA-mNGS in different clinical applications.
Table 1: Diagnostic Performance in Pulmonary Infections and Aspergillosis
| Infection Type / Study Focus | Test Method | Sensitivity/ Detection Rate | Specificity | Key Comparative Findings | Citation |
|---|---|---|---|---|---|
| Non-neutropenic Pulmonary Aspergillosis | BALF cfDNA-mNGS | 89.47% (when combined with CMTs) | Not Specified | cfDNA outperformed wcDNA: Significantly higher Aspergillus RPM values. AUC for predicting true PA was 0.779 (cut-off RPM >4.5). | [21] |
| Non-neutropenic Pulmonary Aspergillosis | BALF wcDNA-mNGS | 84.21% (when combined with CMTs) | Not Specified | Combined with CMTs, both mNGS methods were superior to CMTs alone. | [21] |
| Suspected Pulmonary Infections | BALF cfDNA-mNGS | 91.5% (Detection Rate) | Not Specified | cfDNA superior for low-load pathogens: Detected 31.8% of fungi, 38.6% of viruses, and 26.7% of intracellular microbes missed by wcDNA-mNGS. | [29] |
| Suspected Pulmonary Infections | BALF wcDNA-mNGS | 83.1% (Detection Rate) | Not Specified | Performance for detecting microbes with high loads was similar to cfDNA-mNGS. | [29] |
Table 2: Diagnostic Performance in Sepsis and Body Fluid Infections
| Infection Type / Study Focus | Test Method | Sensitivity/ Detection Rate | Specificity | Key Comparative Findings | Citation |
|---|---|---|---|---|---|
| Early Suspected Infection (Blood) | Plasma cfDNA-mNGS | 74.4% (vs. 12.1% for culture) | Not Specified | Guided therapy change in 70.3% of cases (149/212). Shorter hospital stays with early testing. | [44] |
| Pathogens in Body Fluids (e.g., Ascites, Pleural) | wcDNA-mNGS | 74.07% | 56.34% | wcDNA-mNGS superior to cfDNA-mNGS in body fluids: Higher concordance with culture (63.33% vs 46.67%) and lower host DNA background (84% vs 95%). | [36] |
| Pathogens in Body Fluids (e.g., Ascites, Pleural) | cfDNA-mNGS | Not Specified | Not Specified | The high host DNA background (95%) potentially compromises sensitivity in body fluid samples. | [36] |
| CNS Infections in ICU (CSF) | mNGS (Type unspecified) | 59% | 90.5% | Detected 105 microbial species across 520 samples, identifying 172 infection cases vs. 31 by culture. | [45] |
Detailed Experimental Protocols
To ensure reproducibility and provide clarity on the generated data, this section outlines the standard experimental protocols for wcDNA and cfDNA mNGS as cited in the literature.
Sample Processing and Nucleic Acid Extraction
The fundamental difference between the two methods lies in the initial sample processing and the source of the nucleic acids.
cfDNA Extraction: For bronchoalveolar lavage fluid (BALF) or blood, samples are centrifuged (e.g., 20,000 × g for 15 min) to separate the supernatant. The cfDNA is then extracted from this supernatant using commercial kits, such as the QIAamp DNA Micro Kit (QIAGEN) or the VAHTS Free-Circulating DNA Maxi Kit (Vazyme) [36] [29] [44]. This process avoids the mechanical disruption of human cells, potentially reducing background host DNA.
wcDNA Extraction: The pellet from the initial centrifugation, containing intact human and microbial cells, is subjected to mechanical lysis (e.g., bead-beating with nickel beads) followed by nucleic acid extraction using kits like the QIAamp DNA Mini Kit or QIAamp DNA Micro Kit (QIAGEN) [36] [29]. This method aims to release total genomic DNA but may also increase the co-extraction of host DNA.
Library Construction and Bioinformatics
Following extraction, the workflows converge.
- Library Construction: DNA libraries are prepared from both cfDNA and wcDNA using ultra-low-input library preparation kits, such as the QIAseq Ultralow Input Library Kit (QIAGEN) or the VAHTS Universal Pro DNA Library Prep Kit (Vazyme) [21] [36] [29]. Quality control is performed using instruments like the Agilent 2100 Bioanalyzer or Qubit Fluorometer.
- Sequencing: Qualified libraries are sequenced on platforms like the Illumina Nextseq 550 or NovaSeq [21] [36] [29].
- Bioinformatic Analysis: Raw sequencing data are processed to remove low-quality and short reads. Human sequence data is subtracted by alignment to the human reference genome (e.g., hg38) using tools like Bowtie2. The remaining non-human reads are classified by alignment to microbial genome databases (e.g., NCBI NT database) using BLASTN or similar tools [29] [44] [22]. Positive criteria often involve comparing reads per million (RPM) to negative controls and setting thresholds for genome coverage.
The Researcher's Toolkit
Table 3: Essential Reagents and Kits for mNGS Pathogen Identification
| Research Reagent / Solution | Function / Application | Example Products / Kits |
|---|---|---|
| Nucleic Acid Extraction Kits | Isolation of cfDNA or wcDNA from clinical samples. | QIAamp DNA Micro Kit (QIAGEN), VAHTS Free-Circulating DNA Maxi Kit (Vazyme) [36] [29]. |
| Library Preparation Kits | Construction of sequencing libraries from low-input DNA. | QIAseq Ultralow Input Library Kit (QIAGEN), VAHTS Universal Pro DNA Library Prep Kit (Vazyme) [21] [29]. |
| Sequencing Platforms | High-throughput sequencing of DNA libraries. | Illumina Nextseq 550, Illumina NovaSeq [21] [36] [29]. |
| Bioinformatics Tools | Data QC, host sequence removal, and pathogen identification. | Bowtie2 (host removal), BLASTN (microbial alignment), Kneaddata, Trimmomatic [29] [22]. |
| Microbial Genome Database | Reference database for classifying non-host sequencing reads. | NCBI Nucleotide (NT) Database, custom Pan-genome databases [29] [44]. |
The choice between wcDNA-mNGS and cfDNA-mNGS is highly context-dependent, influenced by the sample type, target pathogens, and the specific clinical question. The consolidated data indicates a trend where cfDNA-mNGS demonstrates superior performance for detecting difficult-to-lyse or intracellular pathogens (like fungi and viruses) in respiratory samples [21] [29] and is the default choice for bloodstream infections (sepsis) [44]. Conversely, wcDNA-mNGS may be more sensitive for typical community-acquired bacteria and in non-respiratory sterile body fluids, such as ascites and pleural fluid, where the high host DNA background in cfDNA can be a limiting factor [36]. For CNS infections, the evidence base is still developing, but mNGS overall shows a clear advantage over culture-based methods [45]. A synergistic diagnostic approach, leveraging the strengths of both mNGS methods alongside conventional microbiological tests, appears to be the most effective strategy for comprehensive pathogen identification in complex clinical cases.
Overcoming Technical Hurdles: Optimization Strategies for Enhanced Sensitivity and Specificity
The effectiveness of metagenomic next-generation sequencing (mNGS) for pathogen identification is significantly compromised by the overwhelming presence of host DNA in clinical samples. This challenge is particularly acute in body fluids like bronchoalveolar lavage fluid (BALF) and blood, where host DNA can constitute over 95% of the total sequenced material, drastically reducing the sensitivity for detecting microbial pathogens [2] [46]. To overcome this barrier, two primary strategic approaches have been developed: the use of different analyte types (whole-cell DNA vs. cell-free DNA) and the implementation of various host depletion techniques. This guide objectively compares these methods, providing a detailed analysis of their performance, experimental protocols, and applications within pathogen identification research.
Analytical Framework: wcDNA vs. cfDNA mNGS
The choice between whole-cell DNA (wcDNA) and cell-free DNA (cfDNA) as the analyte for mNGS represents a fundamental methodological branch, each with distinct advantages and limitations for different clinical scenarios.
- Whole-Cell DNA (wcDNA) mNGS extracts genetic material from intact microbial cells. The process typically involves a bead-beating step to lyse tough microbial cell walls, followed by DNA purification. This method captures DNA from viable microorganisms and is amenable to pre-extraction host depletion techniques, which physically remove or lyse host cells before DNA extraction [29] [1] [28].
- Cell-Free DNA (cfDNA) mNGS targets short fragments of microbial DNA circulating in the supernatant of bodily fluids, which is extracted after a centrifugation step to remove cells. This analyte is particularly useful for detecting hard-to-lyse or intracellular pathogens, as it avoids the biases and inefficiencies of cell lysis [29] [9] [28].
Comparative studies across different sample types and patient populations have yielded critical insights into the performance characteristics of these two approaches. The data below summarizes key findings from recent clinical evaluations.
Table 1: Comparative Performance of wcDNA and cfDNA mNGS in Clinical Studies
| Study (Sample Type) | Sample Size | Performance Metric | wcDNA mNGS | cfDNA mNGS | Reference Standard |
|---|---|---|---|---|---|
| He et al., 2022 [29] [1] (BALF, Pulmonary Infections) | 130 | Detection Rate | 83.1% | 91.5% | Clinical Diagnosis |
| Total Coincidence Rate | 63.9% | 73.8% | Clinical Diagnosis | ||
| Fungi detected only by this method | 19.7% (13/66) | 31.8% (21/66) | mNGS Results | ||
| Viruses detected only by this method | 14.3% (10/70) | 38.6% (27/70) | mNGS Results | ||
| PMC Study 2025 [2] (Body Fluids) | 30 | Concordance with Culture | 63.33% (19/30) | 46.67% (14/30) | Culture |
| Mean Host DNA Proportion | 84% | 95% | Sequencing Data | ||
| Journal of Advanced Research 2024 [28] (Infected Body Fluids) | 248 | ROC AUC (Virus Detection in Blood) | Not Specified | 0.9814 | qPCR/Amplicon NGS |
| ROC AUC (Combined Assay) | 0.7545 (Cellular DNA) | 0.8041 | qPCR/Amplicon NGS |
The data reveals a context-dependent performance. For pulmonary infections, cfDNA mNGS demonstrates a superior detection rate, particularly for fungi, viruses, and intracellular microbes, likely because the genetic material of these pathogens is more readily available in the cell-free fraction [29] [1] [28]. Conversely, in body fluid samples associated with abdominal infections, wcDNA mNGS showed higher concordance with culture results, suggesting it may be more effective for detecting common cultivable bacteria [2]. A key trade-off is the higher proportion of host DNA in cfDNA mNGS, which can reach 95%, thus consuming more sequencing depth [2]. However, combining both analytes has been shown to provide the highest diagnostic efficacy, leveraging the strengths of each method [28].
Pre-Extraction Host Depletion and Filtration Techniques
For wcDNA mNGS, pre-extraction host depletion is a critical step to enrich microbial content before sequencing. These methods leverage physical, chemical, or biochemical differences between host and microbial cells.
Key Methodologies and Workflows
A recent benchmarking study evaluated seven pre-extraction host depletion methods using BALF and oropharyngeal (OP) samples [46]. The following workflow illustrates the general process and the specific mechanisms of each method.
Diagram 1: Workflow of Pre-Extraction Host Depletion Methods for mNGS.
- Nuclease Digestion (R_ase): This method uses a nuclease enzyme to digest free-floating DNA (primarily host-derived cfDNA) in the sample. Intact microbial cells are protected by their cell walls. It showed the highest bacterial DNA retention rate (median 31% in BALF) but relatively low host depletion efficiency [46].
- Osmotic Lysis with PMA or Nuclease (Opma, Oase): A hypotonic solution lyses host cells, which lack sturdy cell walls. The released host DNA is then degraded either by propidium monoazide (PMA), which penetrates only compromised membranes and cross-links DNA upon light exposure, or by nuclease. O_pma was the least effective in increasing microbial reads [46].
- Saponin Lysis with Nuclease (S_ase): The detergent saponin selectively permeabilizes host cell membranes. Subsequent nuclease treatment digests the released host DNA. This method was highly effective, showing the best performance in increasing microbial reads for OP samples (65.60%, 5.9-fold increase) and was among the best for BALF [46].
- Filter-based Enrichment (F_ase): This method, developed in the benchmark study, uses a 10 μm filter to retain host cells while allowing smaller microbial cells to pass through or be washed through. The filtrate is then treated with nuclease to remove any residual host cfDNA. This method demonstrated a balanced and effective performance [46].
- Commercial Kits (Kqia, Kzym): These kits, such as the QIAamp DNA Microbiome Kit (Kqia) and the HostZERO Microbial DNA Kit (Kzym), employ optimized proprietary protocols, often based on selective lysis and digestion. K_zym showed the highest microbial read increase in BALF (2.66% of total reads, 100.3-fold) [46].
Novel Filtration Technologies
Beyond the methods above, a novel Zwitterionic Interface Ultra-Self-assemble Coating (ZISC)-based filtration device (e.g., Micronbrane's Devin filter) has been developed specifically for blood samples [27]. The filter's coating selectively binds and retains host leukocytes and other nucleated cells while allowing bacteria and viruses to pass through unimpeded. In a clinical validation study, this technology achieved >99% white blood cell (WBC) removal. When integrated into a gDNA-based mNGS workflow, it enabled a tenfold increase in microbial reads (average of 9,351 RPM vs. 925 RPM in unfiltered samples) and detected pathogens in 100% of blood culture-positive sepsis samples [27].
Comparative Performance Data of Host Depletion Methods
The effectiveness of host depletion methods can be quantified by their ability to reduce host DNA and increase microbial sequencing reads. The following table synthesizes performance data from key studies.
Table 2: Performance Benchmarking of Host Depletion Methods
| Method | Principle | Host DNA Reduction (vs. Raw) | Microbial Read Increase (vs. Raw) | Key Findings / Best For |
|---|---|---|---|---|
| S_ase [46] | Saponin lysis + Nuclease | 1.1‱ of original (BALF) | 55.8-fold (BALF), 5.9-fold (OP) | High host depletion efficiency; top performer for OP samples. |
| K_zym [46] | Commercial Kit (HostZERO) | 0.9‱ of original (BALF) | 100.3-fold (BALF) | Best microbial read increase in BALF samples. |
| F_ase [46] | 10μm Filtration + Nuclease | Significant reduction | 65.6-fold (BALF) | Balanced performance across all metrics. |
| ZISC Filtration [27] | Coated Filter (Devin) | >99% WBC removal (Blood) | >10-fold (Blood; 9,351 vs. 925 RPM) | gDNA from blood; high sensitivity for sepsis. |
| R_ase [46] | Nuclease Digestion | Significant reduction | 16.2-fold (BALF) | Highest bacterial DNA retention (31% in BALF). |
| O_pma [46] | Osmotic Lysis + PMA | Significant reduction | 2.5-fold (BALF) | Least effective in increasing microbial reads. |
It is crucial to note that all host depletion methods can introduce taxonomic biases. For instance, some methods may significantly diminish the recovery of specific pathogens like Prevotella spp. and Mycoplasma pneumoniae or alter the overall microbial community composition [46]. Furthermore, pre-extraction methods are generally ineffective on frozen samples, as freeze-thaw cycles compromise host cell integrity, rendering selective lysis impossible [46] [47].
The Scientist's Toolkit: Essential Reagents and Kits
Table 3: Key Research Reagents and Kits for Host Depletion and mNGS
| Product / Method | Function / Principle | Application Note |
|---|---|---|
| QIAamp DNA Microbiome Kit (K_qia) | Selective lysis of human cells and degradation of released DNA. | Effective for various sample types; part of a widely used commercial workflow [46]. |
| HostZERO Microbial DNA Kit (K_zym) | Proprietary method for selective host cell removal and DNA depletion. | Showed excellent host depletion and microbial read enrichment in BALF [46]. |
| ZISC-based Filtration Device (Devin) | Physical filtration via a zwitterionic coating that binds host cells. | Specifically designed for enriching microbial cells from whole blood [27]. |
| NEBNext Microbiome DNA Enrichment Kit | Post-extraction method that removes methylated host DNA. | Reported to have poor performance in removing host DNA from respiratory samples [46]. |
| Saponin-Based Lysis (S_ase) | Detergent that selectively permeabilizes eukaryotic membranes. | Highly effective; requires concentration optimization (e.g., 0.025%) [46]. |
| Benzonase Nuclease | Enzyme that degrades all forms of DNA and RNA. | Used in methods like Rase and Sase to digest free-floating host DNA after lysis [46] [47]. |
| Propidium Monoazide (PMA) | DNA intercalating dye that cross-links DNA upon light exposure, inhibiting PCR. | Used in O_pma to selectively degrade DNA from membrane-compromised (host) cells [46]. |
The choice between wcDNA and cfDNA mNGS, and the selection of an appropriate host depletion strategy, are not one-size-fits-all decisions. They must be tailored to the sample type, suspected pathogens, and clinical question. For detecting viruses, fungi, and intracellular pathogens in low-host background samples like BALF, cfDNA mNGS holds a distinct advantage [29] [28]. In contrast, for samples with very high host cellularity, such as blood, wcDNA mNGS coupled with robust pre-extraction host depletion (e.g., ZISC filtration or Sase) provides significantly higher microbial enrichment and sensitivity [46] [27]. The emerging consensus is that a combined approach, utilizing both cfDNA and wcDNA, maximizes diagnostic coverage and efficacy [28]. As the field advances, novel technologies like the ZISC filter and the balanced Fase method offer promising paths toward more sensitive, comprehensive, and unbiased pathogen detection.
Zwitterionic Interface Ultra-Self-assemble Coating (ZISC) filtration represents a significant advancement in host depletion for metagenomic next-generation sequencing (mNGS). This technology effectively addresses the critical challenge of excessive human DNA in clinical samples, which can obscure microbial pathogen detection. By enabling a physical separation of host white blood cells (WBCs) from microbes prior to DNA extraction, ZISC filtration significantly enriches microbial genomic DNA (gDNA) content. When integrated into a whole-cell DNA (wcDNA) mNGS workflow, it demonstrates a clear performance advantage over cell-free DNA (cfDNA) mNGS approaches for pathogen identification in sepsis, leading to a greater than tenfold increase in microbial read counts and achieving 100% detection of expected pathogens in clinical validation [48] [24].
For time-pressed researchers, the table below summarizes the core performance advantages of integrating ZISC filtration into the wcDNA mNGS workflow.
Table 1: Key Performance Advantages of ZISC-Filtered wcDNA mNGS
| Performance Metric | ZISC-Filtered wcDNA mNGS | Unfiltered wcDNA mNGS | cfDNA mNGS |
|---|---|---|---|
| WBC Depletion Efficiency | >99% [48] [24] | Not Applicable | Not Applicable |
| Average Microbial Reads (RPM) in Sepsis | 9,351 RPM [48] [24] | 925 RPM [48] [24] | 1,251 - 1,488 RPM [48] [24] |
| Pathogen Detection Rate (vs. Culture) | 100% (8/8 samples) [48] [24] | Information Missing | 46.67% (14/30 samples) [2] |
| Microbial Composition Preservation | Yes, suitable for accurate profiling [48] [24] | Information Missing | Information Missing |
| Impact on Fungi/Virus Detection | Preserved [24] | Information Missing | Potentially higher for low-load intracellular microbes [1] |
The application of mNGS for pathogen detection in blood samples is fundamentally hampered by the overwhelming abundance of human host DNA. The human genome is approximately 1,000 times larger than a typical bacterial genome and one million times larger than a viral genome. Consequently, even trace amounts of host nucleic acids can consume over 95% of sequencing reads, drastically reducing the sensitivity for detecting pathogenic organisms [40] [49]. Effective host depletion is therefore not merely an optimization step but a prerequisite for sensitive mNGS-based diagnostics.
The choice of starting material—whole-cell DNA (wcDNA) versus cell-free DNA (cfDNA)—presents a critical methodological crossroad. The wcDNA approach, which sequences DNA from intact microbial cells in the blood cell pellet, is amenable to pre-extraction host cell depletion. In contrast, the cfDNA approach sequences microbial DNA fragments found in the plasma, which cannot be enriched using methods that target intact cells [24]. This distinction is central to evaluating the utility of novel host depletion technologies like ZISC filtration.
Experimental Comparison of Host Depletion Methods
Evaluated Techniques and Workflows
The performance of ZISC-based filtration was systematically evaluated against other established host depletion techniques and sequencing approaches. The key methodologies compared in the cited studies are outlined below.
Table 2: Summary of Compared Host Depletion and mNGS Methods
| Method Name | Type | Fundamental Principle | Compatible mNGS Type |
|---|---|---|---|
| ZISC Filtration (Novel) | Pre-extraction, physical | Zwitterionic charge-mediated retention of nucleated host cells; microbes pass through [24] [49]. | wcDNA |
| Differential Lysis (QIAamp Kit) | Pre-extraction, biochemical | Selective lysis of human cells, followed by degradation of released host DNA [24]. | wcDNA |
| CpG Methylation Enrichment (NEBNext Kit) | Post-extraction, biochemical | Binding and removal of CpG-methylated host DNA [24]. | wcDNA |
| Cell-Free DNA (cfDNA) mNGS | N/A | Sequencing of DNA fragments from plasma; no pre-extraction host cell depletion possible [24]. | cfDNA |
| Computational Subtraction | Post-sequencing, bioinformatic | In silico removal of sequencing reads that align to the human reference genome [40]. | wcDNA or cfDNA |
The following diagram illustrates the pivotal position of the host depletion step within the two primary mNGS workflows for blood samples, highlighting the fundamental difference between wcDNA and cfDNA paths.
Quantitative Performance Data
The efficacy of these methods was quantitatively assessed using spiked samples and clinical specimens. The novel ZISC filter demonstrated a white blood cell (WBC) removal efficiency of >99% across varying blood volumes (3-13 mL) without retaining significant quantities of bacteria (e.g., E. coli, S. aureus, K. pneumoniae) or viruses (feline coronavirus), which passed through unimpeded [24].
In a direct comparison using a spiked blood sample, the ZISC-based method proved superior to other techniques. When coupled with Illumina sequencing, it yielded the highest number of microbial reads, demonstrating both high efficiency and a minimal impact on the authentic microbial community structure [24].
The most compelling evidence comes from clinical validation with blood culture-positive sepsis patients. As summarized in Table 1, the use of ZISC filtration in a gDNA-based mNGS workflow led to an average microbial read count of 9,351 reads per million (RPM), a more than tenfold increase over unfiltered gDNA samples (925 RPM). This translated to a 100% (8/8) detection rate for the culture-confirmed pathogens. In the same study, cfDNA-based mNGS showed inconsistent sensitivity and was not significantly enhanced by the filtration step, with RPM values ranging from 1,251 to 1,488 [48] [24].
This performance disparity is supported by a larger, independent study of 30 body fluid samples, which found that wcDNA mNGS had a significantly higher concordance with culture results (63.33%) compared to cfDNA mNGS (46.67%) [2].
Detailed Experimental Protocols
To ensure reproducibility and provide a clear technical reference, this section outlines the key experimental methodologies from the cited studies.
- Sample Preparation: Collect whole blood using sterile technique. For the clinical validation, approximately 4 mL of blood was processed per sample.
- Filtration Setup: Securely connect a sterile syringe to the novel ZISC-based fractionation filter (e.g., Devin Filter, Micronbrane).
- Filtration: Transfer the whole blood sample into the syringe. Gently depress the plunger to push the blood through the filter into a clean collection tube (e.g., 15 mL Falcon tube).
- Critical Note: The gentle pressure ensures that microbial cells are not mechanically damaged and pass through the filter.
- Downstream Processing: The filtrate, now depleted of >99% of WBCs, is then ready for low-speed centrifugation (e.g., 400g for 15 min) to separate plasma from the remaining microbial cell pellet for wcDNA extraction.
- Sample Collection and Division: Collect clinical sample (e.g., Bronchoalveolar Lavage Fluid - BALF, or blood). For blood, proceed with plasma separation as in Figure 1.
- cfDNA Extraction (from plasma or BALF supernatant):
- Centrifuge sample at high speed (e.g., 20,000 × g for 15 min) to pellet cells and debris.
- Transfer the supernatant to a new tube.
- Extract cfDNA from 400 μL of supernatant using a commercial kit (e.g., VAHTS Free-Circulating DNA Maxi Kit), following manufacturer's instructions.
- wcDNA Extraction (from cell pellet):
- Use the precipitate from step 2.
- Add lysing matrix (e.g., nickel beads) and shake vigorously to facilitate cell lysis.
- Extract total DNA from the lysate using a commercial kit (e.g., Qiagen DNA Mini Kit).
- Sequencing and Analysis:
- Prepare sequencing libraries from both cfDNA and wcDNA extracts using identical kits and conditions.
- Sequence on a platform such as Illumina NovaSeq or NextSeq.
- Process data through a standardized bioinformatics pipeline to eliminate human sequences and identify microbial pathogens.
The Scientist's Toolkit: Essential Research Reagents
Successful implementation of these advanced mNGS workflows relies on specific reagents and kits. The table below catalogs key solutions used in the featured experiments.
Table 3: Key Research Reagents for mNGS Host Depletion & Pathogen Detection
| Reagent / Kit Name | Function in Workflow | Specific Application / Note |
|---|---|---|
| Devin Host Depletion Filter (Micronbrane) [24] [49] | Pre-extraction physical depletion of WBCs from whole blood. | Core ZISC technology; enables >99% host cell removal in <2 minutes. |
| ZymoBIOMICS Microbial Community Standards (Zymo Research) [24] | Spike-in control for validating host depletion and detection sensitivity. | Contains defined mixtures of bacteria/fungi at known genome equivalents (GE). |
| VAHTS Free-Circulating DNA Maxi Kit (Vazyme Biotech) [2] | Extraction of cell-free DNA (cfDNA) from plasma or supernatant. | Critical for the cfDNA mNGS workflow. |
| QIAamp DNA Microbiome Kit (Qiagen) [24] | Differential lysis-based host DNA depletion. | Used as a comparator method to ZISC filtration. |
| NEBNext Microbiome DNA Enrichment Kit (NEB) [24] | Post-extraction enrichment of microbial DNA by removing methylated host DNA. | Used as a comparator method to ZISC filtration. |
| Ultra-Low Input Library Prep Kits (e.g., from Vazyme, Qiagen) [2] [24] | Preparation of sequencing libraries from low-abundance DNA extracts. | Essential for handling samples after host depletion where microbial DNA yield can be low. |
The body of evidence demonstrates that ZISC filtration is a highly effective method for mitigating host DNA interference in mNGS. Its primary advantage lies in its operating principle—a charge-based physical separation that is rapid, efficient, and preserves the integrity of diverse microbial populations [24] [49].
When framed within the broader thesis of wcDNA versus cfDNA mNGS, the data strongly supports the conclusion that a wcDNA approach, augmented by robust pre-extraction host depletion like ZISC filtration, is superior for comprehensive pathogen detection in bloodstream infections [48] [2] [24]. While cfDNA mNGS may have a role in detecting intracellular pathogens or in specific clinical scenarios [1], it generally exhibits lower and more inconsistent sensitivity [2]. The integration of ZISC filtration into the wcDNA workflow directly enriches the microbial signal, thereby reducing sequencing costs and improving diagnostic yield, making it a valuable tool for researchers and clinicians aiming to optimize mNGS for pathogen identification.
The accurate identification of pathogens via metagenomic next-generation sequencing (mNGS) is fundamentally dependent on the effectiveness of bioinformatic pipelines in managing two major technical challenges: the predominance of host nucleic acids and the intrusion of contaminant sequences. These pipelines must efficiently filter out human host reads while simultaneously distinguishing true pathogens from background contamination, all of which is influenced by the type of genetic material being sequenced—whole-cell DNA (wcDNA) or cell-free DNA (cfDNA). The choice between wcDNA and cfDNA not only affects wet-lab procedures but also dictates specific bioinformatic strategies for data analysis. This review provides a comparative analysis of experimental and computational approaches for host read removal and contaminant mitigation within the context of pathogen identification, evaluating the performance of wcDNA and cfDNA mNGS across various clinical applications.
Performance Comparison: wcDNA vs. cfDNA mNGS
Clinical studies directly comparing wcDNA and cfDNA mNGS reveal a complex performance landscape where optimal assay choice depends on the sample type, suspected pathogen category, and clinical context. The following data summarizes key comparative studies.
Table 1: Comparative Performance of wcDNA mNGS and cfDNA mNGS Across Clinical Studies
| Sample Type | Study Focus | Key Performance Metrics (wcDNA vs. cfDNA) | Conclusion | Citation |
|---|---|---|---|---|
| Clinical Body Fluids (n=125) | Pathogen ID in abdominal & other infections | Concordance with culture: 63.3% (wcDNA) vs. 46.7% (cfDNA). Host DNA proportion: 84% (wcDNA) vs. 95% (cfDNA). | wcDNA mNGS showed higher sensitivity for pathogen detection in body fluid samples, particularly abdominal infections. | [2] |
| Bronchoalveolar Lavage Fluid (BALF) (n=130) | Diagnosis of pulmonary infections | Detection rate: 83.1% (wcDNA) vs. 91.5% (cfDNA). Exclusive virus detection: 14.3% (wcDNA) vs. 38.6% (cfDNA). Exclusive fungi detection: 19.7% (wcDNA) vs. 31.8% (cfDNA). | cfDNA mNGS is superior for detecting viruses, fungi, and intracellular microbes with low microbial loads. | [29] [1] |
| Cerebrospinal Fluid (CSF) (n=390) | Diagnosis of CNS infections | Overall sensitivity: 32.0% (wcDNA) vs. 60.2% (cfDNA). Exclusive viral detection: 72.6% by cfDNA only. Exclusive mycobacterial detection: 68.8% by cfDNA only. | cfDNA mNGS is significantly more sensitive for CNS infections, especially for viruses and mycobacteria. | [50] |
Analysis of Comparative Performance Data
The data indicates that the superiority of one method over another is context-dependent. The higher sensitivity of wcDNA mNGS in body fluid samples associated with abdominal infections is likely due to the presence of live, intact bacteria, whose genomic DNA is efficiently captured [2]. However, this comes with the trade-off of lower specificity, necessitating careful clinical interpretation to distinguish pathogens from commensals or contaminants.
Conversely, cfDNA mNGS demonstrates a clear advantage in detecting intracellular pathogens (e.g., viruses, mycobacteria) and fungi across pulmonary and CNS infection studies [29] [50]. This is largely because cfDNA represents a snapshot of ongoing microbial activity and cell death, bypassing the need for lysis of hardy cell walls or obligate intracellular organisms. The significantly higher proportion of host DNA in cfDNA samples (95% vs. 84%) underscores the critical need for highly efficient host read filtration bioinformatic pipelines to uncover the diagnostically relevant microbial signal [2].
Experimental Protocols and Methodologies
The differential performance of wcDNA and cfDNA mNGS is rooted in their distinct laboratory workflows, which directly impact the input material for bioinformatic analysis.
Sample Processing and DNA Extraction
The initial steps in processing samples for wcDNA and cfDNA are fundamentally different and are designed to selectively enrich different types of nucleic acid material.
Table 2: Key Research Reagent Solutions in mNGS Workflows
| Item Name | Function in Protocol | Application in wcDNA/cfDNA | |
|---|---|---|---|
| QIAamp DNA Micro Kit (QIAGEN) | Extraction of genomic and cell-free DNA | Used for both wcDNA and cfDNA extraction from various body fluids. | [1] [50] |
| VAHTS Free-Circulating DNA Maxi Kit (Vazyme) | Selective isolation of cell-free DNA | Specifically used for cfDNA extraction from sample supernatant. | [2] |
| Qiagen DNA Mini Kit | Extraction of whole-cell genomic DNA | Used for wcDNA extraction from cell pellets or direct samples. | [2] |
| QIAseq Ultralow Input Library Prep Kit (QIAGEN) | Construction of sequencing libraries from low-input DNA | Essential for cfDNA and low-biomass wcDNA samples. | [1] [50] |
| Dithiothreitol (DTT) | Liquefaction and homogenization of viscous samples | Used in processing sputum and BALF samples prior to nucleic acid extraction. | [51] [52] |
| Benzonase | Enzymatic degradation of host nucleic acids | Used in mNGS workflows to deplete human DNA and increase microbial sequencing depth. | [53] |
The following workflow diagrams illustrate the core experimental protocols for wcDNA and cfDNA mNGS, highlighting the points where host reads and contaminants can be introduced.
Diagram 1: Comparative Experimental Workflow for wcDNA and cfDNA mNGS
Bioinformatic Analysis Pipeline
Following sequencing, raw data undergoes a multi-step computational process to identify microbial pathogens accurately. The following diagram and table detail the standard bioinformatic steps, with a focus on steps critical for managing host and contaminant sequences.
Diagram 2: Core Bioinformatic Pipeline for Host Read Filtration and Pathogen Identification
Table 3: Key Steps in the Bioinformatic Pipeline for Host and Contaminant Management
| Bioinformatic Step | Tool Examples | Function & Rationale | Impact on wcDNA/cfDNA | |
|---|---|---|---|---|
| Quality Control & Adapter Trimming | Fastp | Removes technical sequences and low-quality data to prevent misalignment. | Critical for both; cfDNA fragments are shorter, requiring careful handling. | [29] [51] |
| Host Read Depletion | Bowtie2, BWA, BMTagger | Maps reads to the human reference genome (hg38) and removes them from analysis. | Vital for cfDNA where host DNA can constitute >95% of total reads. Less critical but still important for wcDNA. | [2] [1] [50] |
| Microbial Classification | Kraken, MetaPhlAn2, SNAP | Aligns non-host reads to curated microbial genome databases for taxonomic assignment. | Common to both; database comprehensiveness is key for unbiased detection. | [53] [51] |
| Thresholding & Validation | Pavian, In-house scripts | Applies statistical thresholds (Z-score, RPM ratio) to distinguish true pathogens from background. | Essential for both to mitigate contamination; thresholds may need optimization for each assay type. | [2] [29] |
Critical Analysis of Detection Thresholds and Specificity
A significant challenge in mNGS bioinformatics is establishing criteria that maximize true positive detections while minimizing false positives from contamination or colonization.
Establishing Pathogen Detection Criteria
Studies have implemented rigorous thresholds to determine reportable pathogens. Common criteria include:
- Z-score Comparison: A species' Z-score must be threefold higher than that in negative controls [2].
- Read Count Thresholds: Minimum reads (e.g., >100 for bacteria) are required to ensure signal significance [2].
- Genomic Region Coverage: Reads must map to multiple, distinct genomic regions (e.g., ≥5) to confirm the presence of an organism's genome rather than a conserved, isolated fragment [2].
- Relative Abundance Optimization: Implementing pathogen-specific relative abundance thresholds has been shown to reduce false-positive rates significantly, for example, from 39.7% to 29.5% in one pediatric pneumonia study using targeted NGS [52].
The application of these thresholds must be contextual. The compromised specificity observed in wcDNA mNGS, as reported in one body fluid study, highlights that even with these filters, detecting microbial DNA does not always equate to clinical infection [2]. Bioinformatic pipelines must therefore be coupled with clinical correlation.
The choice between wcDNA and cfDNA mNGS represents a fundamental trade-off that directly shapes bioinformatic strategies for host read filtration and contaminant mitigation. wcDNA mNGS demonstrates superior sensitivity for detecting live, extracellular bacteria in non-sterile sites but struggles with intracellular pathogens and suffers from lower specificity. In contrast, cfDNA mNGS excels in the diagnosis of infections involving viruses, fungi, and mycobacteria in sterile body compartments like the CNS and lungs, despite the challenge of a higher host DNA background.
The wet-lab protocols and bioinformatic pipelines for each method are consequently optimized for different scenarios. Effective pathogen identification relies on a synergistic combination of appropriate sample processing, rigorous host DNA depletion in silico, and the application of validated, context-aware detection thresholds. Future developments in bioinformatics, including machine learning models for integrating clinical metadata with sequencing metrics and standardized, validated thresholds for different sample types and assays, will be crucial for maximizing the clinical utility of both wcDNA and cfDNA mNGS.
Metagenomic next-generation sequencing (mNGS) has emerged as a powerful, hypothesis-free tool for pathogen detection in clinical diagnostics. A critical methodological choice in mNGS workflow is the selection of the nucleic acid source: whole-cell DNA (wcDNA), which sequences DNA from intact microorganisms and host cells, or cell-free DNA (cfDNA), which targets microbial DNA freely circulating in body fluids. Establishing precise diagnostic thresholds for each method is essential for accurate pathogen reporting and minimizing false-positive results. This guide objectively compares the performance of wcDNA-mNGS versus cfDNA-mNGS across various clinical scenarios, providing researchers and clinicians with evidence-based criteria for implementation.
Performance Comparison: wcDNA-mNGS vs. cfDNA-mNGS
The diagnostic performance of wcDNA-mNGS and cfDNA-mNGS varies significantly depending on the sample type, infection site, and target pathogen. The table below summarizes key comparative metrics from recent clinical studies.
Table 1: Comparative Performance of wcDNA-mNGS and cfDNA-mNGS in Pathogen Detection
| Clinical Context (Sample Type) | Comparative Metric | wcDNA-mNGS | cfDNA-mNGS | Reference/Study |
|---|---|---|---|---|
| Body Fluid Samples (Pleural, Ascites, etc.) | Concordance with Culture Results | 63.33% (19/30) | 46.67% (14/30) | Sun et al. [54] [36] |
| Mean Host DNA Proportion | 84% | 95% (p<0.05) | Sun et al. [54] [36] | |
| Sensitivity (vs. Culture) | 74.07% | Not Reported | Sun et al. [54] [36] | |
| Specificity (vs. Culture) | 56.34% | Not Reported | Sun et al. [54] [36] | |
| Viral CNS Infection (CSF) | Sensitivity for Virus Detection | 33.3% (8/24) | 66.7% (16/24) (p<0.01) | PMC10783088 [55] |
| Mean Host DNA Proportion (n=26) | 96% ± 0.08 | 91% ± 0.1 (p<0.01) | PMC10783088 [55] | |
| Non-Neutropenic Pulmonary Aspergillosis (BALF) | Aspergillus RPM (Reads Per Million) | Lower | Significantly Higher | Frontiers in Cellular and Infection Microbiology [43] |
| Suspected Sepsis (Blood) | Overall Pathogen Detection Rate | Not Applicable | 48.8% (83/170) | PMC12188782 [56] |
| Sensitivity (vs. Blood Culture) | Not Applicable | 71.43% | PMC12188782 [56] | |
| Specificity (vs. Blood Culture) | Not Applicable | 55.6% | PMC12188782 [56] |
Experimental Protocols and Diagnostic Thresholds
Sample Processing and Nucleic Acid Extraction
The fundamental difference between the two methods lies in the initial sample processing, which directly influences host DNA contamination and subsequent sensitivity.
wcDNA Extraction Protocol: Clinical body fluid samples (e.g., BALF, CSF) are processed without initial centrifugation. The retained precipitate is subjected to mechanical beating with nickel beads to lyse cells, followed by DNA extraction using kits such as the Qiagen DNA Mini Kit [36] [43]. This method captures DNA from both intact microbes and human cells.
cfDNA Extraction Protocol: Samples are first centrifuged (e.g., 20,000 × g for 15 minutes) to remove human cells and debris. Cell-free DNA is then extracted from the supernatant using specialized kits like the VAHTS Free-Circulating DNA Maxi Kit or the QIAamp DNA Micro Kit [55] [36] [43]. This step aims to enrich for microbial nucleic acids that are freely circulating due to infection.
Establishing Positive Reporting Criteria
To minimize false positives, stringent bioinformatic thresholds must be applied after sequencing and alignment to reference databases. The following criteria, synthesized from multiple studies, provide a framework for pathogen reporting.
Table 2: Key Criteria for Positive Pathogen Reporting in mNGS
| Criterion | Recommended Threshold | Rationale & Technical Notes |
|---|---|---|
| Microbial Read Threshold | >100 reads for bacteria; >10 reads for fungi/viruses [36] | Filters out low-level background noise; thresholds may be adjusted based on pathogen and sample type. |
| z-score (vs. Negative Control) | >3 [36] | Ensures the signal is statistically significant compared to contamination in no-template controls. |
| Genomic Coverage | Reads mapped to ≥3-5 non-overlapping genomic regions [55] [36] | Indicates broad genomic detection, reducing false positives from single-region contamination. |
| RPM Ratio (RPM-r) | ≥10 (RPMsample/RPMNTC) [55] | Normalizes pathogen reads against negative control; crucial for bacteria/fungi to account for reagent contaminants. |
| Genus-to-Species Discernment | Highest species read count must be ≥5-10x greater than other species in the genus [36] | Addresses challenges in differentiating highly conserved genomic regions between related species. |
Workflow Visualization
The following diagram illustrates the parallel pathways for wcDNA and cfDNA mNGS analysis, highlighting key decision points that influence diagnostic thresholds and the risk of false positives.
The Scientist's Toolkit: Essential Research Reagents
Successful implementation of mNGS diagnostics relies on a suite of specialized reagents and tools. The following table details key solutions for method development and validation.
Table 3: Essential Research Reagent Solutions for mNGS Method Development
| Reagent / Solution | Function / Application | Example Kits & Notes |
|---|---|---|
| Nucleic Acid Extraction Kits | Isolate DNA from whole cells or cell-free supernatant. Critical for yield and purity. | wcDNA: Qiagen DNA Mini Kit [36].cfDNA: VAHTS Free-Circulating DNA Maxi Kit, QIAamp DNA Micro Kit [55] [36]. |
| DNA Library Prep Kit | Fragments DNA and adds adapters for sequencing. Essential for NGS compatibility. | VAHTS Universal Pro DNA Library Prep Kit for Illumina [36]. |
| Negative Control (NTC) | Identifies laboratory or reagent-borne contamination for false-positive filtration. | "No template control" water processed identically to clinical samples [55] [36]. |
| Microbial Genome Databases | Reference for aligning sequenced reads to identify pathogens. | NCBI Microbial Genome Databases (ftp://ftp.ncbi.nlm.nih.gov/genomes/) [55]. |
| Bioinformatic Software | Analyzes raw data: host read filtering, pathogen alignment, threshold application. | Tools like Pavian for calculating z-scores and read percentages [36]. Custom pipelines (e.g., DISQVER) [56]. |
| Human Reference Genome | Filters out human host sequences to improve microbial signal detection. | hg38 [55]. |
The choice between wcDNA and cfDNA mNGS is context-dependent, requiring careful consideration of clinical presentation and sample type. wcDNA-mNGS demonstrates higher sensitivity in body fluid infections like abdominal infections, but its lower specificity (56.34%) necessitates rigorous interpretation to avoid false positives [54] [36]. In contrast, cfDNA-mNGS is superior for detecting viral CNS infections and shows enhanced performance for fungal pathogens like Aspergillus in BALF, largely due to its significantly lower host DNA background [55] [43]. Establishing and adhering to strict diagnostic thresholds—including read counts, genomic coverage, and statistical comparison to controls—is paramount for both methods to ensure accurate pathogen reporting and mitigate the risk of false-positive results in clinical practice.
The accurate identification of pathogens through metagenomic next-generation sequencing (mNGS) is fundamentally dependent on the efficient recovery of microbial DNA from clinical specimens. The critical choice between targeting whole-cell DNA (wcDNA) and microbial cell-free DNA (cfDNA) represents a significant methodological crossroads in infectious disease research, with substantial implications for diagnostic sensitivity, specificity, and practical implementation [2] [40] [1]. This comparison guide provides an objective analysis of these competing approaches by synthesizing recent experimental evidence to inform researchers, scientists, and drug development professionals.
The fundamental distinction between these methods lies in their starting material: wcDNA protocols extract nucleic acids from intact microbial cells, often requiring vigorous mechanical or chemical lysis, while cfDNA approaches target microbial DNA fragments already released into sample supernatants [2] [1]. As research continues to expand into low-biomass environments and challenging clinical samples, optimizing DNA recovery through methodological refinements has become increasingly crucial for obtaining reliable, reproducible results.
Performance Comparison: wcDNA mNGS vs. cfDNA mNGS
Comprehensive Performance Metrics
Multiple recent studies have directly compared the performance characteristics of wcDNA and cfDNA mNGS across different sample types and clinical scenarios. The table below summarizes key quantitative findings from controlled comparisons:
Table 1: Direct performance comparison between wcDNA mNGS and cfDNA mNGS
| Performance Metric | wcDNA mNGS | cfDNA mNGS | Study Context | Reference |
|---|---|---|---|---|
| Sensitivity | 74.07% | 46.67% | Body fluid samples (n=30) vs. culture | [2] |
| Specificity | 56.34% | Not reported | Body fluid samples vs. culture | [2] |
| Host DNA Proportion | Mean 84% | Mean 95% | Body fluid samples (n=30) | [2] |
| Detection Rate | 83.1% | 91.5% | Pulmonary infections (n=130) | [1] |
| Total Coincidence Rate | 63.9% | 73.8% | Pulmonary infections vs. conventional methods | [1] |
| Fungi Detection (Exclusive) | 19.7% (13/66) | 31.8% (21/66) | Low-load pathogens in BALF | [1] |
| Viruses Detection (Exclusive) | 14.3% (10/70) | 38.6% (27/70) | Low-load pathogens in BALF | [1] |
| Intracellular Microbes Detection (Exclusive) | 6.7% (2/30) | 26.7% (8/30) | Low-load pathogens in BALF | [1] |
Concordance with Reference Methods
When evaluated against traditional culture methods, wcDNA mNGS demonstrated significantly higher concordance (63.33%, 19/30) compared to cfDNA mNGS (46.67%, 14/30) in body fluid samples [2]. In the same study, wcDNA mNGS also showed greater consistency with bacterial culture results (70.7%, 29/41) compared to 16S rRNA NGS (58.54%, 24/41) [2].
Conversely, in pulmonary infection diagnostics, cfDNA mNGS outperformed wcDNA mNGS in overall detection rate (91.5% vs. 83.1%) and total coincidence rate with clinical diagnoses (73.8% vs. 63.9%) [1]. This apparent contradiction highlights how optimal methodology depends on sample type and target pathogens.
Experimental Protocols for Method Comparison
Sample Processing and DNA Extraction
The fundamental methodological differences begin at the initial sample processing stage:
wcDNA Protocol: Precipitates from body fluid samples are retained through centrifugation (20,000 × g for 15 minutes). The pellet undergoes mechanical lysis using bead-beating with 3-mm nickel beads at 3,000 rpm for 5 minutes, followed by DNA extraction using commercial kits such as the Qiagen DNA Mini Kit [2].
cfDNA Protocol: Supernatants from centrifuged samples are carefully collected, avoiding disruption of the cell pellet. Cell-free DNA is extracted from 400 μL of supernatant using specialized kits designed for low-concentration samples, such as the VAHTS Free-Circulating DNA Maxi Kit [2] or QIAamp DNA Micro Kit [1] [22].
Library Preparation and Sequencing
Both approaches typically proceed through similar downstream workflows once DNA is extracted:
Library Construction: Using kits such as the VAHTS Universal Pro DNA Library Prep Kit for Illumina [2] or QIAseq Ultralow Input Library Kit [1]
Sequencing Platform: Generally performed on Illumina platforms (e.g., NovaSeq) with 2×150 or 2×250 paired-end configurations [2] [1]
Data Generation: Approximately 8 GB of data per sample (∼26.7 million reads) for mNGS, while 16S rRNA NGS typically generates ∼0.05 million reads per sample [2]
Bioinformatic Analysis and Pathogen Reporting
Bioinformatic processing follows standardized pipelines:
- Quality Control: Removal of adapter sequences, low-quality reads, and short reads (<35 bp) [2] [22]
- Host DNA Depletion: Mapping to human reference genome (hg38) using Bowtie2 [2] [22]
- Microbial Identification: Alignment of non-human reads to comprehensive microbial databases using BLASTN or similar tools [2] [1] [22]
Reporting criteria typically incorporate multiple thresholds to distinguish true pathogens from background noise, including:
- z-score ratios compared to negative controls (typically >3)
- Minimum read counts (e.g., >100 for bacteria)
- Genomic region requirements (e.g., mapping to 5 different genomic regions)
- Exclusion of contaminants, colonizers, and commensals based on established criteria [2]
Technical Workflow Comparison
The diagram below illustrates the key procedural differences between wcDNA and cfDNA mNGS workflows:
Optimized Protocol Modifications for Enhanced DNA Recovery
Agar-Containing Solutions for Low-Biomass Samples
Recovering sufficient microbial DNA from low-biomass specimens remains technically challenging. Recent innovations include using agar-containing sampling solutions (0.05-0.4% w/v) that significantly increase microbial DNA recovery from challenging environments like human skin [57]. This approach:
- Increased DNA yield particularly from low-microbial-load sites (volar forearm, antecubital fossa)
- Reduced contamination rates from non-sample microbes
- Functioned as an effective co-precipitant during DNA extraction
- Outperformed conventional sampling solutions (ST and SCF) in quantitative comparisons [57]
The mechanism appears to involve agar's co-precipitant properties during microbial cell and DNA precipitation, with similar efficacy observed with alternative co-precipitants like glycogen and sodium alginate [57].
Mechanical Homogenization Optimization
For wcDNA extraction from tough microbial samples, controlled mechanical homogenization is crucial. The Bead Ruptor Elite system exemplifies how optimized parameters (speed, cycle duration, temperature, bead type) can maximize DNA recovery while minimizing fragmentation [7]. Key considerations include:
- Using specialized bead tubes (ceramic, stainless steel) for different sample types
- Implementing temperature control to reduce heat-induced DNA damage
- Balancing lysis efficiency with DNA shearing concerns
- Processing tough specimens (tissue, bacteria, stool) without harsh chemicals [7]
Modified Sample Preparation for Complex Matrices
Innovative pre-extraction modifications can significantly enhance DNA recovery:
Ceramic Bead Addition: Incorporating 1.4 mm ceramic beads before supernatant removal in subgingival plaque samples improved DNA concentration (23.82 ± 23.31 ng/μL vs. 13.6 ± 17.07 ng/μL in standard methods) and increased Shannon diversity [58].
Combined Mechanical-Chemical Lysis: For extremely challenging samples like bone, a strategic combination of EDTA demineralization with mechanical homogenization improves DNA access while managing PCR inhibition concerns [7].
Research Reagent Solutions
Table 2: Essential research reagents and materials for microbial DNA recovery studies
| Reagent/Material | Function | Example Products/Protocols | Application Context |
|---|---|---|---|
| DNA Extraction Kits | Nucleic acid purification from various sample types | Qiagen DNA Mini Kit, QIAamp DNA Micro Kit, PowerSoil DNA Isolation Kit, PureLink Genomic DNA Mini Kit | wcDNA (pellet), cfDNA (supernatant), low-biomass samples [2] [1] [57] |
| Mechanical Homogenization | Cell disruption for DNA release | Bead Ruptor Elite with ceramic/stainless steel beads | Tough samples (bacteria, tissue, stool); improves lysis efficiency [7] [58] |
| Agar-Containing Solutions | Enhanced DNA recovery from low-biomass samples | 0.2% agar in sampling solution | Skin microbiome, other low-biomass environments; acts as co-precipitant [57] |
| Library Preparation Kits | Sequencing library construction from low-input DNA | VAHTS Universal Pro DNA Library Prep Kit, QIAseq Ultralow Input Library Kit | Compatible with low DNA concentrations from clinical samples [2] [1] |
| Host DNA Depletion Reagents | Reduce human background in microbial sequencing | Not specified in results | Critical for samples with high host:microbe DNA ratios [40] |
Discussion and Research Implications
The comparative data reveals a nuanced landscape for method selection in microbial DNA recovery. The higher sensitivity of wcDNA mNGS for bacterial pathogens in body fluids [2] must be balanced against the superior performance of cfDNA mNGS for detecting fungi, viruses, and intracellular microbes at low loads [1].
For researchers designing studies involving challenging samples, several strategic considerations emerge:
Sample Type Dictates Method Choice: Body fluids from sterile sites may favor wcDNA approaches, while pulmonary samples might benefit from cfDNA protocols.
Target Pathogen Influences Protocol: Studies focusing on intracellular microbes, fungi, or viruses may achieve better results with cfDNA mNGS despite its generally lower overall sensitivity for bacteria.
Biomass Level Guides Optimization: Low-biomass samples require specialized enhancements like agar-containing solutions or optimized bead-beating parameters.
The compromised specificity of wcDNA mNGS (56.34% compared to culture) highlighted in body fluid studies [2] underscores the importance of careful interpretation and integration with complementary diagnostic methods. This limitation necessitates rigorous contamination controls and validated reporting thresholds in research settings.
Future directions should focus on hybrid approaches that leverage the strengths of both methods, particularly for complex clinical scenarios like polymicrobial infections or immunocompromised patients where comprehensive pathogen detection is critical. Additionally, continued refinement of mechanical lysis parameters and specialized sampling solutions will further enhance DNA recovery from the most challenging sample types.
Data-Driven Comparison: Analytical Validation and Clinical Performance Metrics
Metagenomic Next-Generation Sequencing (mNGS) has emerged as a powerful, hypothesis-free tool for pathogen detection, capable of identifying bacteria, viruses, fungi, and parasites without prior knowledge of the causative agent [40]. Unlike traditional diagnostic methods that rely on specific culturing conditions or targeted molecular assays, mNGS sequences all nucleic acids in a sample, providing a comprehensive view of the microbial landscape [40]. This capability is particularly valuable for detecting fastidious, slow-growing, or novel pathogens that often elude conventional methods [2] [40].
Two primary approaches have been developed for sample processing in mNGS: whole-cell DNA (wcDNA) and cell-free DNA (cfDNA) methods. The wcDNA approach extracts nucleic acids from intact microbial cells, potentially capturing a broader spectrum of living organisms. In contrast, the cfDNA method targets microbial DNA fragments circulating in body fluids, which may represent actively shedding or lysing pathogens [1] [59]. The choice between these approaches significantly impacts diagnostic performance, with varying sensitivities and specificities reported across different sample types and clinical scenarios.
This guide provides a systematic comparison of wcDNA mNGS and cfDNA mNGS performance against culture and PCR, presenting quantitative data, detailed methodologies, and analytical frameworks to inform research applications and clinical development.
Performance Metrics: Quantitative Comparison
The diagnostic performance of wcDNA mNGS and cfDNA mNGS varies significantly across different clinical specimens and pathogen types. The table below summarizes key performance metrics from recent studies.
Table 1: Comparative Performance of wcDNA mNGS and cfDNA mNGS Across Sample Types
| Sample Type | Method | Sensitivity (%) | Specificity (%) | Reference Standard | Key Findings |
|---|---|---|---|---|---|
| Clinical Body Fluids (n=125) | wcDNA mNGS | 74.07 | 56.34 | Culture [2] | Significantly higher sensitivity for abdominal infections |
| cfDNA mNGS | 46.67 | N/R | Culture [2] | Lower concordance with culture results | |
| Pulmonary Infections (BALF, n=130) | wcDNA mNGS | 83.1* | N/R | Composite clinical diagnosis [1] | Lower detection rate for fungi, viruses, and intracellular microbes |
| cfDNA mNGS | 91.5* | N/R | Composite clinical diagnosis [1] | Superior for low-load pathogens | |
| Viral CNS Infections (CSF, n=26) | wcDNA mNGS | 33.3 | N/R | Clinical diagnosis [59] | Higher human DNA background |
| cfDNA mNGS | 66.7 | N/R | Clinical diagnosis [59] | Lower human DNA interference (0.91±0.1 vs 0.96±0.08, p<0.01) | |
| Infected Pancreatic Necrosis (Meta-analysis) | wcDNA mNGS | 87 | 83 | Clinical diagnosis [60] | AUC: 0.92 |
| Culture | 36 | 83 | Clinical diagnosis [60] | Significantly lower sensitivity (p<0.05) |
*Detection rate rather than formal sensitivity calculation N/R = Not Reported
A meta-analysis of mNGS for infectious diseases including 20 studies and 2,716 participants reported an overall pooled sensitivity of 75% (95% CI: 72-77%) and specificity of 68% (95% CI: 66-70%) when compared to various reference standards [61]. The area under the summary receiver operating characteristic curve (AUC) was 0.85, indicating excellent overall performance [61].
Table 2: Pathogen-Type Detection Performance
| Pathogen Type | wcDNA mNGS Advantage | cfDNA mNGS Advantage |
|---|---|---|
| Gram-negative Bacteria | Better detection of Enterobacteriaceae and non-fermenting bacteria (79.2% detection rate) [22] | |
| Gram-positive Bacteria | Lower detection rate (22.2%) compared to culture [22] | |
| Fungi | 31.8% detected only by cfDNA vs 19.7% only by wcDNA in BALF [1] | |
| Viruses | 38.6% detected only by cfDNA vs 14.3% only by wcDNA in BALF [1] | |
| Intracellular Microbes | 26.7% detected only by cfDNA vs 6.7% only by wcDNA in BALF [1] | |
| Atypical Pathogens | Limited detection | Superior for Mycobacterium, Clostridium tetanus, and parasites [22] |
Experimental Protocols and Methodologies
Sample Processing Workflows
The fundamental difference between wcDNA and cfDNA mNGS lies in sample preparation. The following diagram illustrates the divergent workflows:
DNA Extraction Protocols
wcDNA Extraction Method: The wcDNA protocol begins with vigorous mechanical lysis using nickel beads or similar materials to break open microbial cells [2] [1]. The precipitated sample is shaken at 3,000 rpm for 5 minutes with beads, followed by DNA extraction using commercial kits such as the Qiagen DNA Mini Kit [2]. This method aims to recover DNA from intact microorganisms but may also release substantial human DNA from host cells in the sample.
cfDNA Extraction Method: The cfDNA approach utilizes supernatant after high-speed centrifugation (20,000 × g for 15 minutes) to remove intact cells and debris [2] [59]. Cell-free DNA is extracted from 400μL of supernatant using specialized kits like the VAHTS Free-Circulating DNA Maxi Kit or QIAamp DNA Micro Kit [2] [23]. This process enriches for freely circulating microbial DNA while reducing background human DNA.
Sequencing and Bioinformatics
Both methods typically employ Illumina platforms (NovaSeq or NextSeq) for high-throughput sequencing [2] [1] [23]. For wcDNA mNGS, approximately 8GB of data (26 million reads) per sample is generated, while cfDNA mNGS may require adjusted sequencing depths due to lower human background [2].
Bioinformatic analysis follows a standardized pipeline:
- Quality Control: Removal of adapter sequences and low-quality reads using tools like Trimmomatic [23]
- Host Depletion: Mapping to human reference genome (hg38) using Bowtie2 to remove human sequences [1] [23]
- Microbial Identification: Alignment to comprehensive microbial databases using BLASTN or similar tools [1] [23]
- Contamination Filtering: Implementation of z-score thresholds and comparison with negative controls to identify contaminants [2]
The Scientist's Toolkit: Essential Research Reagents
Table 3: Key Reagents and Kits for mNGS Research
| Reagent/Kits | Function | Example Applications |
|---|---|---|
| Qiagen DNA Mini Kit | Whole-cell DNA extraction from pellets | wcDNA extraction from body fluids, BALF [2] [1] |
| VAHTS Free-Circulating DNA Maxi Kit | Cell-free DNA extraction from supernatant | cfDNA extraction from CSF, BALF, preservation fluids [2] |
| QIAamp DNA Micro Kit | Cell-free DNA extraction from low-volume samples | cfDNA extraction from drainage fluids, plasma [22] [23] |
| VAHTS Universal Pro DNA Library Prep Kit | Library preparation for Illumina platforms | Both wcDNA and cfDNA library construction [2] |
| QIAseq Ultralow Input Library Kit | Library preparation from low-input DNA | cfDNA library construction from limited samples [1] |
Interpretation Guidelines and Clinical Applications
Performance Optimization Strategies
The choice between wcDNA and cfDNA mNGS should be guided by the clinical or research question:
Choose wcDNA mNGS when:
- Suspecting Gram-negative bacteria or typical pathogens [22]
- Working with abdominal infections or sterile body fluids [2]
- Cost-effectiveness is a priority (single extraction method)
Choose cfDNA mNGS when:
- Suspecting viral, fungal, or intracellular pathogens [1] [59]
- Working with CSF for CNS infections [59] [30]
- Low microbial biomass is suspected
- Reduced host background is critical for sensitivity
Diagnostic Integration Framework
Neither wcDNA nor cfDNA mNGS should be viewed as a standalone replacement for conventional methods. The optimal diagnostic approach incorporates:
- Parallel Testing: Combining mNGS with culture and PCR maximizes detection capabilities [22] [40]
- Result Validation: Subthreshold mNGS findings should be confirmed with orthogonal methods [30]
- Clinical Correlation: Integration with patient symptoms, immune status, and exposure history [40]
Recent large-scale implementation data from a 7-year study of 4,828 CSF samples demonstrates the real-world performance of mNGS, with an overall sensitivity of 63.1% and specificity of 99.6% for CNS infections, outperforming indirect serologic testing (28.8% sensitivity) and direct detection testing from CSF (45.9% sensitivity) [30].
The comparative analysis of wcDNA and cfDNA mNGS reveals a complex performance landscape where neither method universally outperforms the other. wcDNA mNGS demonstrates superior sensitivity for bacterial pathogens in body fluids, while cfDNA mNGS excels in detecting viruses, fungi, and intracellular pathogens with reduced host background interference. The integration of both approaches with conventional diagnostic methods, guided by clinical context and pathogen suspicions, represents the most effective strategy for comprehensive pathogen detection in research and clinical development settings.
Metagenomic Next-Generation Sequencing (mNGS) has emerged as a powerful, hypothesis-free tool for pathogen identification. A critical methodological consideration in clinical mNGS is the choice of input nucleic acid material, primarily between whole-cell DNA (wcDNA), which sequences DNA from intact cells, and cell-free DNA (cfDNA), which sequences microbial DNA freely circulating in body fluids. This guide provides an objective, data-driven comparison of wcDNA mNGS versus cfDNA mNGS, synthesizing recent clinical evidence to inform researchers and drug development professionals on their respective performances in key statistical parameters including concordance rates, microbial read counts, and host DNA proportions.
Performance Comparison: wcDNA mNGS vs. cfDNA mNGS
The comparative analytical and diagnostic performance of wcDNA mNGS and cfDNA mNGS varies significantly across different sample types and clinical scenarios. The table below summarizes key quantitative metrics from recent studies.
Table 1: Comparative Performance of wcDNA mNGS and cfDNA mNGS Across Clinical Specimens
| Sample Type | Metric | wcDNA mNGS | cfDNA mNGS | Citation |
|---|---|---|---|---|
| Clinical Body Fluids | Concordance with Culture | 63.33% (19/30) | 46.67% (14/30) | [2] |
| Mean Host DNA Proportion | 84% | 95% | [2] | |
| Sensitivity (vs. Culture) | 74.07% | Not Reported | [2] | |
| Specificity (vs. Culture) | 56.34% | Not Reported | [2] | |
| Bronchoalveolar Lavage Fluid (BALF) | Detection Rate | 83.1% | 91.5% | [1] [62] |
| Total Coincidence Rate | 63.9% | 73.8% | [1] | |
| Exclusive Virus Detection | 14.3% (10/70) | 38.6% (27/70) | [1] | |
| Exclusive Fungus Detection | 19.7% (13/66) | 31.8% (21/66) | [1] | |
| Cerebrospinal Fluid (CSF) | Sensitivity for Viruses | 33.3% (8/24) | 66.7% (16/24) | [59] |
| Mean Human DNA Proportion | 96% | 91% | [59] |
Experimental Protocols and Workflows
Understanding the divergent sample processing protocols is essential for interpreting the performance data in Table 1.
Key Methodological Differences
The fundamental difference lies in the initial sample processing steps, which dictate the source of the genetic material being sequenced.
wcDNA mNGS Workflow: This method targets DNA from intact microbial cells. The standard protocol involves:
- Sample Processing: Clinical samples (e.g., BALF, body fluids) are centrifuged to create a pellet. The pellet is subjected to mechanical (e.g., bead-beating) and/or enzymatic lysis to break open microbial and human cells [2] [1].
- DNA Extraction: Total DNA is extracted from this lysate, containing a mixture of host and microbial genomic DNA [2].
cfDNA mNGS Workflow: This method targets DNA released by microbes into the extracellular environment.
- Sample Processing: The clinical sample is centrifuged at high speed (e.g., 20,000 × g for 15 minutes) to remove intact cells, including human cells and microbial cells [2] [59].
- DNA Extraction: Cell-free DNA is extracted exclusively from the acellular supernatant, which is enriched for freely circulating microbial nucleic acids [2] [1].
The subsequent steps of library preparation, sequencing, and bioinformatic analysis are broadly similar for both approaches, though specific kits and parameters may vary.
Workflow Visualization
The following diagram illustrates the key divergent pathways in sample preparation for wcDNA and cfDNA mNGS.
The Scientist's Toolkit: Essential Research Reagents
Successful implementation of mNGS assays requires specific reagents and kits for nucleic acid extraction, library preparation, and sequencing. The following table details key solutions used in the cited studies.
Table 2: Essential Research Reagents for mNGS Workflows
| Reagent Category | Product Name | Primary Function in mNGS | Representative Use |
|---|---|---|---|
| cfDNA Extraction | VAHTS Free-Circulating DNA Maxi Kit (Vazyme) | Extracts cell-free DNA from plasma or supernatant. | Body fluid cfDNA extraction [2] |
| QIAamp DNA Micro Kit (Qiagen) | Extracts trace amounts of DNA, including cfDNA. | BALF & preservation fluid cfDNA extraction [22] [1] | |
| wcDNA Extraction | Qiagen DNA Mini Kit (Qiagen) | Extracts total genomic DNA from cell pellets. | Body fluid wcDNA extraction [2] |
| Library Preparation | VAHTS Universal Pro DNA Library Prep Kit for Illumina (Vazyme) | Prepares sequencing libraries from double-stranded DNA. | Library construction for body fluid mNGS [2] |
| QIAseq Ultralow Input Library Kit (Qiagen) | Constructs libraries from very low input DNA. | Library construction for BALF mNGS [1] | |
| Nextera XT DNA Library Prep Kit (Illumina) | Prepares multiplexed sequencing libraries. | Library construction for blood mNGS [63] | |
| Sequencing Platform | Illumina NovaSeq / NextSeq | High-throughput short-read sequencing. | Used across multiple studies [2] [63] |
| Bioinformatics | Kraken2 / Bracken | For taxonomic classification of sequencing reads. | Pathogen identification in blood mNGS [63] |
| BLASTN (NCBI) | For aligning sequences to reference databases. | Pathogen identification in tissue/BALF [22] [1] |
The choice between wcDNA and cfDNA mNGS is not universally prescriptive but should be guided by the clinical question and sample type. The data consistently show that wcDNA mNGS demonstrates higher concordance with culture in body fluids, likely because it detects intact, often viable, microorganisms [2]. However, this comes at the cost of a high host DNA background, which can reduce sensitivity for low-abundance pathogens by consuming sequencing depth [2] [14].
In contrast, cfDNA mNGS excels in specific scenarios by targeting unencumbered microbial nucleic acids. Its superior performance in detecting viruses, fungi, and intracellular bacteria in BALF and CSF is linked to its ability to capture pathogens that are difficult to lyse or that reside within host cells [1] [59]. The lower host DNA proportion in CSF cfDNA further enhances its sensitivity for challenging diagnoses like viral CNS infections [59].
In conclusion, wcDNA and cfDNA mNGS are complementary methodologies. wcDNA may be preferable for routine bacterial detection where culture correlation is valued. cfDNA is a powerful tool for immunocompromised patients, cases of suspected viral/fungal/intracellular infection, and when conventional tests are negative. Future research integrating both approaches on a single sample or utilizing metatranscriptomics may provide the most comprehensive diagnostic picture.
The precise identification of pathogens in polymicrobial and low-biomass infections represents a significant challenge in clinical microbiology. Traditional culture-based methods frequently yield false-negative results for fastidious, intracellular, or slow-growing microorganisms, potentially delaying appropriate antimicrobial therapy. Metagenomic next-generation sequencing (mNGS) has emerged as a powerful, hypothesis-free diagnostic tool capable of detecting a broad spectrum of pathogens directly from clinical samples. However, the optimal sample processing strategy—targeting microbial cell-free DNA (cfDNA) versus whole-cell DNA (wcDNA)—remains a subject of active investigation, with each approach exhibiting distinct advantages depending on the clinical context [64].
This comparative assessment synthesizes recent evidence to evaluate the performance characteristics of cfDNA mNGS and wcDNA mNGS for pathogen detection. The analysis focuses specifically on their respective capabilities to resolve complex polymicrobial infections and identify pathogens present in low abundance, two scenarios where conventional diagnostic methods often prove inadequate. By examining experimental data across diverse sample types and clinical syndromes, this guide provides researchers and drug development professionals with an evidence-based framework for selecting appropriate methodologies for specific diagnostic challenges.
Theoretical Foundations and Biological Basis
The fundamental difference between cfDNA and wcDNA mNGS lies in the origin and processing of the nucleic acid material targeted for sequencing. Understanding these biological and technical distinctions is crucial for interpreting performance variations across different clinical applications.
Whole-cell DNA (wcDNA) is extracted from complete microbial cells and intracellular pathogens present in a clinical sample. This method typically involves mechanical or enzymatic lysis of all cells in the specimen—both microbial and human—followed by DNA purification. Consequently, wcDNA preparations often contain significant amounts of background human DNA, which can dominate sequencing libraries and reduce sensitivity for microbial detection unless host depletion strategies are employed [54] [2]. The wcDNA approach theoretically captures the entire microbial repertoire within a sample, including intact cells and intracellular pathogens.
Microbial cell-free DNA (cfDNA) represents short fragments of microbial DNA released into body fluids through microbial cell death, lysis, or active secretion. For sample processing, clinical specimens are centrifuged to remove intact cells, and DNA is extracted exclusively from the supernatant [41] [64]. This process inherently reduces the proportion of background human genomic DNA derived from host cells, potentially enriching for microbial sequences. Circulating mcfDNA fragments typically range from 40-100 base pairs with a half-life of just a few minutes, reflecting active processes of release and clearance [64].
The following diagram illustrates the fundamental differences in the origin and processing pathways for wcDNA and cfDNA:
Performance Comparison Across Sample Types
Body Fluid Infections
A 2025 comparative study analyzing 125 clinical body fluid samples (including pleural, pancreatic, drainage, ascites, and cerebrospinal fluid) provided direct evidence of performance characteristics between wcDNA and cfDNA approaches. Using culture results as a reference standard, wcDNA mNGS demonstrated significantly higher concordance (63.33%) compared to cfDNA mNGS (46.67%) [54]. The mean proportion of host DNA in wcDNA mNGS was 84%, substantially lower than the 95% observed in cfDNA mNGS (p < 0.05), suggesting more efficient capture of microbial signals despite higher absolute host DNA [54] [2].
When compared against 16S rRNA NGS in 41 samples, wcDNA mNGS showed superior consistency with culture results for bacterial detection (70.7% vs. 58.54%) [54]. The calculated sensitivity and specificity of wcDNA mNGS for pathogen detection in body fluid samples were 74.07% and 56.34%, respectively, highlighting its detection capability while acknowledging limitations in specificity that necessitate careful clinical interpretation [54] [2].
Table 1: Performance Comparison in Body Fluid Samples (n=125)
| Parameter | wcDNA mNGS | cfDNA mNGS | 16S rRNA NGS | Reference Method |
|---|---|---|---|---|
| Concordance with culture | 63.33% (19/30) | 46.67% (14/30) | 58.54% (24/41) | Culture [54] |
| Consistency in bacterial detection | 70.7% (29/41) | Not reported | 58.54% (24/41) | Culture [54] |
| Mean host DNA proportion | 84% | 95% (p < 0.05) | Not applicable | N/A [54] [2] |
| Sensitivity | 74.07% | Not reported | Not reported | Culture [54] |
| Specificity | 56.34% | Not reported | Not reported | Culture [54] |
Pulmonary Infections
In contrast to body fluid findings, pulmonary infection studies demonstrate a potential advantage for cfDNA mNGS in certain contexts. A comprehensive analysis of 130 patients with suspected pulmonary infections revealed that mNGS of cfDNA from bronchoalveolar lavage fluid (BALF) achieved a higher detection rate (91.5%) compared to mNGS of wcDNA (83.1%) and conventional methods (26.9%) [29] [65].
Notably, cfDNA mNGS demonstrated particular strength in detecting fungi (31.8% detected only by cfDNA vs. 19.7% only by wcDNA), viruses (38.6% vs. 14.3%), and intracellular microbes (26.7% vs. 6.7%) present in low abundance [29]. After stratifying microbes by reads per million (RPM) thresholds to approximate microbial load, researchers found that cfDNA mNGS identified more microbes classified as low biomass (RPM < 100), while both methods performed similarly for high-abundance pathogens [29].
A 2024 study focusing on non-neutropenic pulmonary aspergillosis further reinforced the value of BALF cfDNA mNGS, reporting that it generated significantly greater RPM values for Aspergillus detection compared to wcDNA mNGS [21]. Receiver operating characteristic (ROC) analysis demonstrated that an RPM threshold greater than 4.5 for Aspergillus detected by BALF-cfDNA predicted "true positive" pulmonary aspergillosis with an AUC of 0.779 [21].
Table 2: Performance Comparison in Pulmonary Infections
| Parameter | cfDNA mNGS | wcDNA mNGS | Conventional Methods | Study |
|---|---|---|---|---|
| Overall detection rate | 91.5% | 83.1% | 26.9% | Frontiers in Cellular and Infection Microbiology 2022 [29] |
| Total coincidence rate | 73.8% | 63.9% | 30.8% | Frontiers in Cellular and Infection Microbiology 2022 [29] |
| Fungi exclusively detected | 31.8% (21/66) | 19.7% (13/66) | Not reported | Frontiers in Cellular and Infection Microbiology 2022 [29] |
| Viruses exclusively detected | 38.6% (27/70) | 14.3% (10/70) | Not reported | Frontiers in Cellular and Infection Microbiology 2022 [29] |
| Intracellular microbes exclusively detected | 26.7% (8/30) | 6.7% (2/30) | Not reported | Frontiers in Cellular and Infection Microbiology 2022 [29] |
| Aspergillus RPM (mean) | Significantly greater | Lower | N/A | Frontiers in Cellular and Infection Microbiology 2024 [21] |
Central Nervous System (CNS) Infections
The diagnostic challenge of CNS infections is particularly acute due to typically low pathogen loads in cerebrospinal fluid and the critical nature of these infections. A comprehensive evaluation of 394 CSF samples from patients with CNS infections revealed markedly superior performance for cfDNA mNGS, which demonstrated a sensitivity of 60.2% (95% CI: 55.1%-65.0%) compared to 32.0% (95% CI: 24.8%-40.2%) for wcDNA mNGS and 20.9% (95% CI: 16.2%-26.5%) for conventional methods [41].
Viral and mycobacterial pathogens, which often present with particularly low biomass in CSF, were predominantly detected by cfDNA mNGS, with 72.6% of viral pathogens and 68.8% of mycobacterial pathogens identified exclusively through this method [41]. This pattern underscores the particular advantage of cfDNA for challenging CNS infections where conventional methods frequently yield negative results despite clear clinical evidence of infection.
Experimental Methodologies
Sample Processing and DNA Extraction
The fundamental methodological differences between cfDNA and wcDNA protocols begin immediately after sample collection:
cfDNA Extraction Protocol [2] [41]:
- Centrifuge clinical samples at 20,000 × g for 15 minutes to pellet intact cells
- Transfer supernatant to new tube, avoiding disturbance of pellet
- Extract cfDNA from 400 μL supernatant using specialized kits (e.g., VAHTS Free-Circulating DNA Maxi Kit, QIAamp DNA Micro Kit)
- Purify DNA following manufacturer's instructions, typically including proteinase K digestion, binding to magnetic beads, washing, and elution
wcDNA Extraction Protocol [2] [29]:
- For body fluids: Use pellet from centrifugation step; for BALF: process directly without centrifugation
- Add mechanical disruption components (e.g., nickel beads) to sample
- Shake at 3,000 rpm for 5 minutes to facilitate comprehensive cell lysis
- Extract DNA from lysate using commercial kits (e.g., Qiagen DNA Mini Kit)
- Purify DNA through standard column-based or magnetic bead-based methods
The following workflow diagram illustrates the key methodological differences:
Sequencing and Bioinformatic Analysis
Library Preparation and Sequencing [2] [21]:
- DNA library construction using commercial kits (e.g., VAHTS Universal Pro DNA Library Prep Kit, QIAseq Ultralow Input Library Kit)
- Quality assessment using Qubit Fluorometer and Agilent Bioanalyzer
- Sequencing on Illumina platforms (NovaSeq, NextSeq) with 2 × 150 bp or 2 × 250 bp configurations
- Approximately 8 GB data (26 million reads) per sample for mNGS; lower depth for 16S rRNA NGS
Bioinformatic Processing [2] [22] [41]:
- Quality control: Remove adapter sequences, filter low-quality reads (<35 bp)
- Host DNA depletion: Map reads to human reference genome (hg38) using Bowtie2
- Microbial classification: Align non-human reads to comprehensive microbial databases (NCBI nt database)
- Pathogen reporting: Apply criteria including z-score comparisons to negative controls, minimum read counts, and genomic coverage requirements
The Scientist's Toolkit: Essential Research Reagents
Table 3: Key Research Reagent Solutions for mNGS Studies
| Reagent/Kit | Function | Application | Representative Study |
|---|---|---|---|
| QIAamp DNA Micro Kit | Nucleic acid extraction | cfDNA and wcDNA extraction from various body fluids | [22] [41] [21] |
| VAHTS Free-Circulating DNA Maxi Kit | cfDNA-specific extraction | Optimized isolation of cell-free DNA from supernatant | [2] |
| Qiagen DNA Mini Kit | Whole-cell DNA extraction | Comprehensive DNA extraction from cell pellets | [2] |
| VAHTS Universal Pro DNA Library Prep Kit | Library preparation | Construction of sequencing libraries for Illumina platforms | [2] |
| QIAseq Ultralow Input Library Kit | Library preparation from low-input DNA | Optimal performance with limited starting material | [29] [41] |
| Illumina NovaSeq/NextSeq Platforms | High-throughput sequencing | Generation of sequencing data (typically 8-40 million reads) | [2] [29] |
| Pavian | Bioinformatic analysis | Calculation of percentage read counts and z-scores | [2] |
| Bowtie2 | Sequence alignment | Removal of host reads by mapping to human genome | [29] [22] |
| BLASTN | Taxonomic classification | Alignment of reads against microbial databases | [22] |
The comparative assessment of wcDNA and cfDNA mNGS approaches reveals a context-dependent performance profile rather than absolute superiority of either method. wcDNA mNGS demonstrates advantages in general body fluid infections and bacterial detection, showing higher sensitivity and better concordance with culture methods. Conversely, cfDNA mNGS excels in specific scenarios including pulmonary infections (particularly for fungi, viruses, and intracellular pathogens), central nervous system infections, and low-biomass situations where it outperforms both wcDNA mNGS and conventional diagnostic methods.
For researchers and drug development professionals, these findings suggest that methodological selection should be guided by the specific clinical question and sample type. The integration of both approaches may provide complementary diagnostic information in complex cases, particularly for immunocompromised patients or those with negative conventional workups. Future methodological refinements in host DNA depletion, targeted enrichment, and bioinformatic analysis will likely enhance the performance of both approaches, further solidifying the role of mNGS in the diagnostic landscape for challenging infections.
Agreement with 16S rRNA NGS and Other Targeted Molecular Methods
The accurate identification of pathogens is fundamental to clinical microbiology, influencing diagnosis, treatment, and patient outcomes. Within the broader thesis comparing whole-cell DNA metagenomic next-generation sequencing (wcDNA mNGS) and cell-free DNA mNGS (cfDNA mNGS) for pathogen identification, this guide provides an objective comparison of 16S ribosomal RNA gene next-generation sequencing (16S rRNA NGS) against these and other molecular methods. We summarize key performance metrics from recent studies, detail standard experimental protocols, and provide resources to inform researchers and drug development professionals.
Performance Data Comparison
The following tables summarize quantitative data from recent studies that directly compare the clinical performance of 16S rRNA NGS with other targeted molecular methods.
Table 1: Comparative Sensitivity and Specificity of Diagnostic Methods
| Diagnostic Method | Sensitivity (%, [95% CI]) | Specificity (%, [95% CI]) | Study Context | Citation |
|---|---|---|---|---|
| Culture (Reference) | 36.36% [26.94–46.64] | 100% [85.75–100] | Various clinical samples (n=123) | [66] |
| 16S rRNA NGS | 68.69% [58.59–77.64] | 87.50% [67.64–97.34] | Various clinical samples (n=123) | [66] |
| Plasma cfDNA mNGS | 62.07% | 57.14% | Bloodstream infections (n=43 sample pairs) | [67] |
Table 2: Concordance and Detection Rates Across Methodologies
| Comparison | Concordance with Culture | Additional Key Findings | Citation |
|---|---|---|---|
| 16S rRNA NGS vs. Culture | 54.47% (67/123 samples) | 16S NGS detected pathogens in 42 culture-negative samples from confirmed infections. | [66] |
| wcDNA mNGS vs. Culture | 70.7% (29/41 samples) | Higher sensitivity for pathogen detection in clinical body fluid samples. | [2] |
| 16S rRNA NGS vs. Culture | 58.54% (24/41 samples) | Lower consistency with culture compared to wcDNA mNGS. | [2] |
| wcDNA mNGS vs. cfDNA mNGS | wcDNA mNGS: 63.33% (19/30)cfDNA mNGS: 46.67% (14/30) | wcDNA mNGS showed higher concordance with culture results. | [2] |
| Plasma mNGS vs. Blood Culture | Detected 78.26% of Gram-negative rods and 17% of Gram-positive cocci. | Plasma is more suitable for mNGS than whole blood; higher detection rate for Gram-negative bacteria. | [67] |
Experimental Protocols
To ensure reproducibility and provide a clear basis for comparison, this section outlines the standard methodologies employed in the studies cited.
16S rRNA NGS Workflow
The 16S rRNA NGS protocol is an amplicon-based sequencing method that targets the bacterial 16S rRNA gene [68].
- DNA Extraction: Total genomic DNA is extracted from clinical samples (e.g., body fluids, tissue) using commercial kits, such as the Qiagen DNA Mini Kit [2]. The extracted DNA includes both host and microbial whole-cell DNA.
- PCR Amplification: The hypervariable regions of the 16S rRNA gene (e.g., V3-V4) are amplified using universal primers (e.g., 341F and 806R) [67] [2].
- Library Preparation: The amplified products are purified, and sequencing adapters are added. Kits such as the VAHTS Universal Pro DNA Library Prep Kit for Illumina are commonly used [67] [2].
- Sequencing: The prepared libraries are sequenced on a next-generation platform, such as the Illumina NovaSeq or Ion PGM, typically with a 2x250 paired-end configuration for sufficient overlap and resolution [2] [66].
- Bioinformatic Analysis:
- Quality Control: Raw reads are processed to remove low-quality sequences and sequencing adapters using tools like Fastp [67].
- Taxonomic Classification: Clean reads are classified against curated 16S rRNA databases (e.g., GreenGenes) using tools like Kraken2 or BLAST [68] [67]. The analysis can be refined with custom algorithms, such as the Cheryblast+ob wrapper, for specific diagnostic applications like pneumonia [69].
mNGS Workflows (wcDNA and cfDNA)
Metagenomic sequencing involves non-targeted sequencing of all nucleic acids in a sample [2].
- Sample Processing and DNA Extraction:
- For wcDNA mNGS: The clinical sample is lysed, and total DNA (host and microbial) is extracted directly from the pellet or uncentrifuged sample using a DNA extraction kit [2].
- For cfDNA mNGS: The sample (e.g., plasma or body fluid supernatant) is centrifuged at high speed (e.g., 20,000 × g). Cell-free DNA is then extracted from the supernatant using a specialized cfDNA kit, such as the VAHTS Free-Circulating DNA Maxi Kit [2].
- Library Preparation: The extracted DNA is fragmented, end-repaired, and ligated with sequencing adapters. For samples with RNA viruses, an initial reverse transcription step to create cDNA is required [67].
- Sequencing: Libraries are sequenced on a platform like the Illumina NovaSeq, generating tens of millions of reads per sample (e.g., 8 GB of data) to achieve sufficient depth for detecting low-abundance pathogens [67] [2].
- Bioinformatic Analysis:
- Host DNA Depletion: Reads aligning to the host reference genome (e.g., GRCh38) are removed using aligners like BWA-MEM [67].
- Microbial Identification: The remaining non-host reads are classified against comprehensive genomic databases using taxonomic profilers like Kraken2. Pathogens are reported based on strict criteria, including read counts, z-scores compared to negative controls, and alignment to multiple genomic regions [67] [2].
Diagram 1: Comparative experimental workflows for 16S rRNA NGS, wcDNA mNGS, and cfDNA mNGS.
The Scientist's Toolkit
Table 3: Essential Research Reagent Solutions
| Item | Function/Application | Specific Examples |
|---|---|---|
| Nucleic Acid Extraction Kits | Isolation of high-quality DNA from diverse sample matrices. | Qiagen DNA Mini Kit (wcDNA) [2]; VAHTS Free-Circulating DNA Maxi Kit (cfDNA) [2]; GenElute Bacterial Genomic DNA Kit [70]. |
| 16S rRNA Amplification Primers | Target-specific amplification of variable regions for taxonomic profiling. | 341F/806R (V3-V4 region) [67]; 27F/337R (V1-V2 region); 337F/518R (V3 region) [70]. |
| Library Preparation Kits | Preparation of sequencing-ready libraries from amplified or genomic DNA. | VAHTS Universal Pro DNA Library Prep Kit for Illumina [67] [2]. |
| Sequencing Platforms | High-throughput sequencing of prepared libraries. | Illumina NovaSeq, MiSeq [67] [2]; Ion Torrent PGM [66]. |
| Bioinformatic Tools | Data processing, quality control, taxonomic classification, and functional analysis. | Fastp (quality control) [67]; BWA-MEM (host read removal) [67]; Kraken2 (taxonomic classification) [67]; BLAST (sequence alignment) [69]; MOTHUR (microbial community analysis) [70]. |
| Reference Databases | Curated genomic databases for accurate taxonomic assignment of sequencing reads. | GreenGenes [68]; NCBI Nucleotide database [71] [69]. |
Method Selection and Logical Workflow
The choice between 16S rRNA NGS, wcDNA mNGS, and cfDNA mNGS depends on the specific research question, sample type, and required resolution. The following diagram outlines a logical decision-making workflow.
Diagram 2: A logical workflow for selecting the appropriate molecular diagnostic method.
The integration of metagenomic next-generation sequencing (mNGS) into clinical microbiology has revolutionized pathogen detection by enabling unbiased identification of microorganisms without prior knowledge of the causative agent. However, a critical methodological question remains unresolved: whether to target microbial cell-free DNA (cfDNA) or whole-cell DNA (wcDNA) for optimal diagnostic performance. Recent studies (2024-2025) have yielded conflicting findings, with some advocating for cfDNA and others for wcDNA, depending on the clinical context. This synthesis examines the emerging evidence to provide a balanced perspective on this methodological debate, offering researchers and clinicians a framework for selecting appropriate sequencing approaches based on specific clinical scenarios and target pathogens.
Comparative Performance Data Across Clinical Specimens
Quantitative Analysis of Recent Studies
Table 1: Comparative performance of cfDNA mNGS versus wcDNA mNGS across different specimen types
| Specimen Type | Study (Year) | Sensitivity/Detection Rate | Specificity | Key Advantages | Notable Limitations |
|---|---|---|---|---|---|
| Body Fluids (pleural, pancreatic, ascites, CSF) | Sun et al. (2025) [2] [54] | wcDNA: 74.07%cfDNA: 46.67% | wcDNA: 56.34% | wcDNA: Higher sensitivity for abdominal infections | wcDNA: Compromised specificity |
| Bronchoalveolar Lavage Fluid (BALF) | He et al. (2022) [29] [1] | cfDNA: 91.5%wcDNA: 83.1% | Not specified | cfDNA: Superior for fungi, viruses, intracellular microbes | wcDNA: May miss low-load pathogens |
| Cerebrospinal Fluid (CSF) | Frontiers in Cellular and Infection Microbiology (2022) [41] | cfDNA: 60.2%wcDNA: 32.0% | Not specified | cfDNA: Better for viral and mycobacterial CNS infections | wcDNA: Significantly lower sensitivity |
| Pulmonary Aspergillosis (BALF) | Frontiers in Cellular and Infection Microbiology (2024) [43] [21] | BALF-cfDNA + CMTs: 89.47%BALF-wcDNA + CMTs: 84.21%CMTs alone: 47.37% | Not specified | cfDNA: Higher Aspergillus reads per million (RPM) | Both require combination with CMTs for optimal performance |
Analysis of Conflicting Findings
The evidence reveals a clear pattern of context-dependent performance. For body fluid samples associated with abdominal infections, wcDNA mNGS demonstrates significantly higher sensitivity (74.07%) compared to cfDNA mNGS (46.67%) when using culture results as a reference [2]. Conversely, in respiratory specimens (BALF), cfDNA mNGS shows superior detection rates (91.5% vs. 83.1%) and is particularly advantageous for identifying fungi, viruses, and intracellular microbes with low pathogen loads [29] [1]. Similarly, for CNS infections, cfDNA mNGS substantially outperforms wcDNA mNGS (60.2% vs. 32.0% sensitivity) [41].
This divergence likely stems from fundamental differences in sample composition and pathogen biology across anatomical sites. Body fluids may contain a higher proportion of intact microbial cells, favoring wcDNA approaches, while respiratory and CNS specimens may have greater representation of microbial cfDNA from host immune activity.
Detailed Experimental Protocols
Nucleic Acid Extraction Methods
Table 2: Key research reagents and their functions in mNGS workflows
| Research Reagent | Manufacturer | Function in Protocol |
|---|---|---|
| QIAamp DNA Micro Kit | QIAGEN | Extraction of both cfDNA and wcDNA from clinical samples |
| VAHTS Free-Circulating DNA Maxi Kit | Vazyme Biotech | Specific extraction of cell-free DNA from supernatant |
| Qiagen DNA Mini Kit | Qiagen | Extraction of whole-cell DNA from precipitated cellular fraction |
| VAHTS Universal Pro DNA Library Prep Kit for Illumina | Vazyme Biotech | DNA library preparation for sequencing |
| QIAseq Ultralow Input Library Kit | QIAGEN | Library construction from low-input DNA samples |
cfDNA Extraction Protocol
For cfDNA extraction, clinical samples (BALF, CSF, or body fluids) are first centrifuged at 20,000 × g for 15 minutes to separate cellular components [2]. The supernatant is carefully collected, avoiding disturbance of the pellet. cfDNA is then extracted from 400 μL of supernatant using the VAHTS Free-Circulating DNA Maxi Kit (Vazyme Biotech) or QIAamp DNA Micro Kit (QIAGEN) [2] [43]. The protocol involves adding 25 μL of Proteinase K, 800 μL of Buffer L/B, and 15 μL of magnetic beads to the sample, followed by brief mixing and incubation at room temperature for 5 minutes. The tube is placed on a magnetic rack to clear the solution, after which the supernatant is removed. After washing steps, 50 μL of elution buffer is added to resuspend the magnetic beads before transferring the supernatant to a new tube [2].
wcDNA Extraction Protocol
For wcDNA extraction, the retained precipitate from the initial centrifugation is utilized. Two 3-mm nickel beads are added to the precipitate, which is then shaken at 3,000 rpm for 5 minutes to facilitate mechanical cell lysis [2]. Subsequently, wcDNA is extracted from the lysed precipitate using the Qiagen DNA Mini Kit according to the manufacturer's protocol [2]. For some BALF samples, wcDNA extraction is performed directly without centrifugation using a bead-beating method for cell disruption [29].
Library Preparation and Sequencing
DNA library preparation is performed using the VAHTS Universal Pro DNA Library Prep Kit for Illumina (Vazyme Biotech) or QIAseq Ultralow Input Library Kit (QIAGEN) [2] [43]. Library quality is assessed using the Qubit Fluorometer and Agilent 2100 Bioanalyzer. Qualified libraries are sequenced on Illumina platforms (NovaSeq or NextSeq 550) using either paired-end 150 bp (PE150) or single-end 75 bp (SE75) configurations [2] [43] [21]. Approximately 8-20 million reads per sample are generated, balancing cost and detection efficiency [72].
Bioinformatic Analysis
Raw sequencing data undergoes quality control to remove adapter sequences and low-quality reads. Human sequences are excluded by mapping to the human reference genome (hg38) using Bowtie2. The remaining clean reads are aligned to microbial genome databases from NCBI using classification tools such as Kraken2 or IDseq [29] [72]. Pathogen reporting thresholds typically include: z-score ratios >3 compared to negative controls, reads mapped to multiple genomic regions, and minimum read counts (e.g., >100 for bacteria, >10 for fungi/viruses) [2].
Methodological Decision Framework
Pathogen-Specific Performance Considerations
The comparative effectiveness of cfDNA versus wcDNA mNGS varies significantly by pathogen type. cfDNA mNGS demonstrates particular advantages for detecting intracellular pathogens (26.7% detected only by cfDNA vs. 6.7% only by wcDNA), viruses (38.6% vs. 14.3%), and fungi (31.8% vs. 19.7%) [29]. This enhanced detection likely occurs because these pathogens release their nucleic acids into the extracellular environment or reside within host cells that are removed during cfDNA extraction, reducing background interference.
For conventional bacterial pathogens, wcDNA mNGS shows strong performance, particularly in body fluid samples where it achieved 70.7% consistency with culture results compared to 58.54% for 16S rRNA NGS [2]. The mechanical lysis steps in wcDNA extraction may more effectively release bacterial DNA from thick cell walls.
Specimen-Specific Recommendations
Technical Considerations and Optimization Strategies
Host DNA Background
A critical factor influencing detection sensitivity is the proportion of host DNA in sequenced material. wcDNA mNGS demonstrates a significantly lower mean host DNA proportion (84%) compared to cfDNA mNGS (95%) [2]. This difference arises because cfDNA extracts from supernatant still contain substantial human cfDNA, potentially diluting microbial signals. For wcDNA protocols, the initial centrifugation step removes some host cells, partially enriching for microbial content in the pellet.
Sequencing Depth and Configuration
Recent optimization studies indicate that 20 million reads in SE75 mode represents the best balance between detection performance and cost-effectiveness [72]. While increasing dataset sizes and read lengths enhances pathogen detection, the marginal benefits diminish beyond this threshold while economic costs and computational time increase substantially. Samples with adequate pathogenic nucleic acid loads show less variability in detection efficiency across different sequencing strategies [72].
The synthesis of recent evidence (2024-2025) reveals that the choice between cfDNA and wcDNA mNGS is highly context-dependent, with neither approach universally superior. cfDNA mNGS demonstrates clear advantages for respiratory infections, CNS infections, and when targeting fungi, viruses, or intracellular pathogens. Conversely, wcDNA mNGS shows better performance for body fluid samples associated with abdominal infections and for detecting typical bacterial pathogens. The methodological decision framework presented herein provides guidance for researchers and clinicians to select the optimal approach based on clinical scenario, specimen type, and suspected pathogens. Future studies exploring integrated approaches that combine both methods or implement targeted host DNA depletion may further enhance the diagnostic utility of mNGS in clinical practice.
Conclusion
The choice between wcDNA and cfDNA for mNGS is not a matter of one being universally superior, but rather dependent on the specific clinical and research context. Recent evidence confirms that wcDNA mNGS often demonstrates higher sensitivity in body fluid samples from abdominal infections, while cfDNA mNGS shows a distinct advantage in detecting viruses in CNS infections, as well as fungi and intracellular pathogens in pulmonary infections, due to its lower host DNA background. The implementation of novel host-depletion techniques, such as ZISC filtration, significantly enhances wcDNA performance, bridging this gap. For the future, the path forward lies not in a single-method approach but in context-driven selection or the complementary use of both DNA sources. Future research should focus on standardizing protocols, developing integrated bioinformatic tools, and conducting large-scale prospective clinical trials to firmly establish the clinical utility and cost-effectiveness of each approach, ultimately paving the way for more precise and personalized infectious disease diagnostics.
References
- 1. Comparison of metagenomic next-generation sequencing ... [https://www.frontiersin.org/journals/cellular-and-infection-microbiology/articles/10.3389/fcimb.2022.1042945/full]
- 2. Comparative analysis of metagenomic next-generation ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC11934473/]
- 3. Multi-biome analysis identifies distinct gut microbial ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC11603027/]
- 4. DNA Extraction Guide: Mastering 7 Essential Sample Types [https://www.thermofisher.com/blog/life-in-the-lab/dna-extraction-guide-mastering-7-essential-sample-types/]
- 5. Phenol-Chloroform-Isoamyl Alcohol DNA Extraction [https://www.protocols.io/view/phenol-chloroform-isoamyl-alcohol-dna-extraction-g2zxbyf7p.html]
- 6. A rapid and high-yield method for nucleic acid extraction [https://www.nature.com/articles/s41598-025-95226-0]
- 7. How to Work with Challenging or Limited Genomic ... [https://blog.omni-inc.com/blog/how-to-work-with-challenging-or-limited-genomic-samples-updated-for-2025]
- 8. Putative Origins of Cell-Free DNA in Humans - PubMed Central [https://pmc.ncbi.nlm.nih.gov/articles/PMC7662960/]
- 9. cfDNA or Genomic DNA-Based mNGS Assays [https://micronbrane.com/cell-free-or-genomic-dna-based-mngs-assays/]
- 10. An in vitro CRISPR screen of cell-free DNA identifies ... [https://www.nature.com/articles/s42003-024-06129-1]
- 11. Cell-free DNA analysis in current cancer clinical trials [https://www.nature.com/articles/s41416-021-01696-0]
- 12. Cell-Free DNA, Tumor Molecular Concordance, and ... [https://www.sciencedirect.com/science/article/pii/S1525157825001412]
- 13. Clinical applications of metagenomics next-generation ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC11199093/]
- 14. Metagenomic Next-Generation Sequencing in Infectious ... [https://www.mdpi.com/2075-4418/15/16/1991]
- 15. Metagenomic next-generation sequencing facilitates precision ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC12588935/]
- 16. Metagenomic next-generation sequencing for concurrent ... [https://www.nature.com/articles/s41598-025-18812-2]
- 17. Rapid metagenomic sequencing for surveillance of ... [https://nanoporetech.com/document/rapid-sequencing-metagenomics-sqk-rpb114-24]
- 18. Multiplex metagenomic sequencing for rapid viral pathogen ... [https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-025-11952-w]
- 19. Metagenomic Sequencing Data: Step-by-Step Guide From ... [https://www.cd-genomics.com/resource-how-analyze-metagenomic-sequencing-data.html]
- 20. Integrative workflows for metagenomic analysis - PMC [https://pmc.ncbi.nlm.nih.gov/articles/PMC4237130/]
- 21. The value of metagenomic next-generation sequencing with ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC11317373/]
- 22. Comparison of pathogen detection performance between ... [https://www.frontiersin.org/journals/cellular-and-infection-microbiology/articles/10.3389/fcimb.2025.1563962/full]
- 23. Comparison of pathogen detection performance between ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC12375685/]
- 24. Optimization of Metagenomic Next-Generation Sequencing ... [https://link.springer.com/article/10.1007/s40291-025-00797-3]
- 25. Clinical value of metagenomic next-generation sequencing in ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC8884048/]
- 26. Impact of Host DNA and Sequencing Depth on the ... [https://www.frontiersin.org/journals/microbiology/articles/10.3389/fmicb.2019.01277/full]
- 27. Optimization of Metagenomic Next-Generation Sequencing ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC12436562/]
- 28. Clinical evaluation of cell-free and cellular metagenomic ... [https://www.sciencedirect.com/science/article/pii/S2090123223000681]
- 29. Comparison of metagenomic next-generation sequencing ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC9684712/]
- 30. Seven-year performance of a clinical metagenomic next- ... [https://www.nature.com/articles/s41591-024-03275-1]
- 31. Clinical evaluation of cell-free and cellular metagenomic ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC10770109/]
- 32. Sample Prep and Cell Isolation Methods for Single-cell [https://frontlinegenomics.com/cell-prep-possibilities-sample-prep-and-cell-isolation-methods-for-single-cell/]
- 33. Ultra-broad hybrid capture-based targeted next-generation sequencing for sensitive plasma pathogen cfDNA detection in bloodstream infections | Journal of Translational Medicine | Full Text [https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-025-07258-9]
- 34. Exploring genetic alterations in circulating tumor DNA from cerebrospinal fluid of pediatric medulloblastoma | Scientific Reports [https://www.nature.com/articles/s41598-021-85178-6]
- 35. Clinical application value of simultaneous plasma and ... [https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-024-10292-5]
- 36. Comparative analysis of metagenomic next-generation sequencing for pathogenic identification in clinical body fluid samples | BMC Microbiology | Full Text [https://bmcmicrobiol.biomedcentral.com/articles/10.1186/s12866-025-03887-8]
- 37. The Role of microRNAs and Cell-Free DNAs in Fungal ... [https://www.mdpi.com/2309-608X/11/10/718]
- 38. Cell-free DNA analysis in healthy individuals by next- ... [https://www.nature.com/articles/s41419-019-1770-3]
- 39. Next-generation sequencing in cancer diagnosis and ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC12009796/]
- 40. Metagenomic Next-Generation Sequencing in Infectious ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC12384723/]
- 41. Metagenomic next-generation sequencing of cell-free and ... [https://www.frontiersin.org/journals/cellular-and-infection-microbiology/articles/10.3389/fcimb.2022.951703/full]
- 42. Role of plasma and blood-cell co-metagenomic ... [https://www.sciencedirect.com/science/article/pii/S0163445325000283]
- 43. The value of metagenomic next-generation sequencing ... [https://www.frontiersin.org/journals/cellular-and-infection-microbiology/articles/10.3389/fcimb.2024.1398190/full]
- 44. Metagenomic next-generation sequencing of plasma cell-free ... [https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-024-09043-3]
- 45. Clinical metagenomic next-generation sequencing test for ... [https://www.sciencedirect.com/science/article/pii/S1201971225003169]
- 46. Benefits and challenges of host depletion methods in ... [https://www.nature.com/articles/s41522-025-00762-2]
- 47. High-resolution microbiome analysis of host-rich samples ... [https://www.nature.com/articles/s41522-025-00851-2]
- 48. Optimization of Metagenomic Next-Generation Sequencing ... [https://pubmed.ncbi.nlm.nih.gov/40670871/]
- 49. Devin Host Depletion Filters - Improve Metagenomics Results [https://micronbrane.com/devin-mngs-host-depletion-filters/]
- 50. Metagenomic next-generation sequencing of cell-free and ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC9551220/]
- 51. The Comparison of Metagenomic Next-Generation ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC9586124/]
- 52. Comparative and clinical impact of targeted next ... [https://www.frontiersin.org/journals/microbiology/articles/10.3389/fmicb.2025.1590792/full]
- 53. Comparative diagnostic performance of metagenomic and ... [https://www.nature.com/articles/s41598-025-11834-w]
- 54. analysis of metagenomic next-generation sequencing for... Comparative [https://pubmed.ncbi.nlm.nih.gov/40128686/]
- 55. Metagenomic next-generation sequencing of cell-free DNA for ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC10783088/]
- 56. Detection of pathogenic microorganisms using ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC12188782/]
- 57. Recovery of microbial DNA by agar-containing solution ... [https://www.nature.com/articles/s41598-023-46890-7]
- 58. Impact of optimised sample preparation method on DNA ... [https://www.sciencedirect.com/science/article/pii/S000399692500127X]
- 59. Metagenomic next-generation sequencing of cell-free DNA ... [https://www.sciencedirect.com/org/science/article/pii/S2165049723004079]
- 60. A Systematic Review and Meta-Analysis [https://link.springer.com/article/10.1007/s10620-025-09474-1]
- 61. Diagnostic accuracy of metagenomic next-generation ... [https://www.nature.com/articles/s41598-022-25314-y]
- 62. Comparison of metagenomic next-generation sequencing ... [https://doaj.org/article/c312673f814248489d340912988a83a3]
- 63. Metagenomic next-generation sequencing in detecting ... [https://www.nature.com/articles/s41390-023-02776-y]
- 64. a focus on microbial cell-free DNA sequencing [https://www.thno.org/v10p5501.htm]
- 65. of metagenomic next-generation sequencing using... Comparison [https://www.bohrium.com/paper-details/comparison-of-metagenomic-next-generation-sequencing-using-cell-free-dna-and-whole-cell-dna-for-the-diagnoses-of-pulmonary-infections/817369810236080128-7347]
- 66. Performance of 16S rRNA Gene Next-Generation ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC11240331/]
- 67. Comparison of metagenomic next-generation sequencing and ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC10847245/]
- 68. 16S and ITS rRNA Sequencing | Identify bacteria & fungi with NGS [https://www.illumina.com/areas-of-interest/microbiology/microbial-sequencing-methods/16s-rrna-sequencing.html]
- 69. A systematic algorithm using 16S ribosomal RNA for ... [https://www.nature.com/articles/s41598-025-14841-z]
- 70. Frontiers | Comparison of 16S rRNA Gene Based Microbial Profiling Using Five Next-Generation Sequencers and Various Primers [https://www.frontiersin.org/journals/microbiology/articles/10.3389/fmicb.2021.715500/full]
- 71. Performance and Application of 16S rRNA Gene Cycle ... [https://pmc.ncbi.nlm.nih.gov/articles/PMC7484979/]
- 72. The effects of sequencing strategies on Metagenomic ... [https://www.sciencedirect.com/science/article/pii/S240584402409460X]